Introduction
We are going to talk about the examination of the upper extremity and how to use that in your treatment planning. This is part of a two-course series that will provide clinical assessment tools and guidelines to aid in the treatment planning for the upper extremity involved patient. Today, we are going to talk about the first half of your assessment of this population.
Why Is An Evaluation Important?
- Establish baselines
- Determine components to be addressed in the treatment/establish a treatment plan
- Determine limitations
- Establish treatment goals
- Determine treatment results and outcomes
- Efficacy of treatment
Obviously, we have to do an evaluation before we do any types of treatment. We need to establish a baseline of where we are starting. We need to determine the components that you are going to address to establish your treatment plan. Even though we have to determine what components are limiting this individual, we are not going to treat just the components, and that is important to keep in mind. You need to determine what the limitations are. How is it limiting them functionally? Then, we need to use our evaluation to establish treatment goals, to determine treatment results and outcomes through reevaluation, and to determine if your treatment is effective or not.
Examination Criteria
- Accurate
- Standard methods
- Reliable
- Reproducible
- Valid
- Needs to be meaningful to your outcome
Your examination methods need to have some specific criteria in order for the results to be meaningful. They need to be accurate and include standard methods that anybody can replicate and use. They need to be reliable, which means that it is stable across time. It needs to be reproducible so that if another therapist is going to do the same test, they can get the same type of results. It should be valid, which means that it is accurately measuring what it is supposed to measure. And, it needs to be meaningful to your outcome. If there is a limitation in an extremity, but it has nothing to do with this patient being able to use their hand, then it is probably not a meaningful measure that you need to be spending your time on.
Documentation
- Concise
- Clear
- Accurate
- Measurable
- Photographs
- Electronic: format
- Pros
- Cons
After you perform your evaluation, you have to document the results. The documentation needs to be concise and clear so that if some other therapist, the attending surgeon, or an outside person, such as an insurance claims adjuster, can read your documentation and understand what you have done, why you have done it, and what it means to this patient. It also needs to be measurable. You can use photographs if you need to. Especially when for wound care assessments, photographs can be very helpful.
Currently, many companies use electronic formats, which is great and not-so-great. The good thing about electronic formats is that they are standardized. Anybody can come in and fill in the blanks. A con with a lot of the electronic formats is that you do not get any of the extraneous information. You can be so intent on filling in your blanks, you may forget to ask some questions or take a measurement that is not on your preformed format. You need to make sure that there is room for your narrative in the electronic formats. I have been involved in the development of some of the electronic formats, and they really do not like to leave room for narrative. As therapists, we love to fill in a narrative. If they do have a narrative, they may limit the number of characters you can put in there so make sure that you are documenting what is important to the client and their goals.
Evaluation
- Evaluation = observation + subjective + examination + conclusion + recommendations
- Need a systematic examination process
What is an evaluation or an examination? You will often hear these terms used interchangeably. Your evaluation is a combination of several things. Your evaluation includes observation skills that you use when your patient first walks in as they are doing everything during that assessment. It is also the subjective component of what they have either filled out on forms or what they have told you verbally. It is also your physical examination. This is you taking actual measurements or palpations of their extremity. It is then all of the information that you gather. They may have limited motion, but what does it mean? Does it limit them functionally? Or is it just limited motion? And then, what your recommendations are regarding treatment. Your recommendations would include the goals that you have established. You should have a systematic examination process that comes back to one of the pros of a formatted, systematic evaluation.
Screening: Subjective
First comes a screening. This is subjective and is based on what the client tells you. It can be either a questionnaire that they complete prior to coming to see you, what you gather during the interview or a combination of the two, which is what most of us do in the clinic. The subjective part is very important. Many therapists have patients fill out forms prior to their appointment, and then, they do not review that. If you are getting the information via a written format prior to coming back into the clinic, make sure you review that information prior to seeing the patient.
Personal Information
- Age, hand dominance, occupation, hobbies, medications
Your subjective information needs to have personal information. This includes the age of the patient, male or female, hand dominance, occupation, hobbies, medications, and that generic personal information, that hopefully, you are getting on every patient. You need to get a picture of who this person is.
History
- Date of injury, surgery
- Onset of symptoms
- Diagnostics performed
- Previous treatment
Then, you are going to find out why they are in your clinic. Are they here because of an injury, a surgery, or something that has been more chronic and ongoing? You want to get the actual date of injury and a description of the injury. You want to get surgical information as well. Did they have surgery? When did they have it? Who performed it? And if you are not in the clinic with those physicians, then you also need to find out if you can obtain a surgery report. You need to know the onset of their symptoms if it is a more chronic type of condition. What diagnostics have been performed and what are the results? If the patient is not sure, then you should contact your referral source to make sure that you obtain that information prior to implementing any treatment. Clients are not reliable sometimes so it is good to get this confirmation. You also want to know about any previous treatment they have received, either professional treatment for this diagnosis or even self-treatment. Find out the specifics on what they have had done and what type of response they had to those interventions. And, sometimes they have tried some things on their own at home prior to seeking treatment, and that is just as important.
Full Medical History
- Other conditions or illnesses
- Alcohol or tobacco use
- Nutrition
You need to find out their full medical history, or a systems review. This is what it is called now. This includes any other conditions or illnesses that may affect either their tolerance to treatment or their healing, which may affect their outcomes. Alcohol and tobacco use are very important to note, along with nutrition. These things are going to affect their ability to heal and recover and participate in treatment.
Functional Limitations
- ADLs
- Work
- Hobbies
- School activities
- Sports
- Have them keep a journal if unsure.
What are their functional limitations? They cannot just be coming in because they have pain only, and if their pain is not limiting them. Most patients will be coming in because they have limitations. They are not able to do what they need to do to complete their daily activities. To find out about ADLs, you may have to prompt them. I will go through all their tasks like dressing, bathing, grooming, and meal preparation. I will cue them to see if there is something that they are not thinking about. What type of work do they do? Are they having limitations at work? What type of hobbies do they engage in? Some people take their hobbies very seriously so you need to make sure and find out about that. If it is a younger person, are they in school? Is it limiting their school activities? Is it limiting their participation in sports? A lot of patients cannot, on the spot, tell you where their limitations are. During the initial eval, they may tell me, "Well, it just kind of bothers me." I will then have them keep a journal before they return for their second visit so that I can get the specifics. The reason this is important is that I want to establish functional goals. For me to establish a functional goal, it cannot be what I think they need to do. It needs to be what they need to be able to return to. The other reason I do this is I want to make sure that their goals and limitations are real. Depending on the injury, they may want to get back to a sport that is going to be very challenging so I need to know that up front.
Symptoms (Objectify)
- Pain, numbness tingling, weakness, deformity, impaired coordination
- When
- Duration
- Where
- Interfere with activity
- Interfere with sleep
Again, they may have already filled out some of their symptoms prior to coming back to see you. Please make sure and review first. Are they having pain, numbness and tingling in the extremity? Are they encountering any weakness? Is there a deformity that seems to limit or bother them? Even if it bothers them psychologically, that can also be limiting. It may keep them from participating in social activities because they do not like the way something looks. Do they have impaired coordination? Is it limiting their ability to open containers, buttons, or close fasteners?
When they are having their symptoms, I want a little more specifics. When are they having them? How long does it last? Where are their symptoms, specifically? When they give that whole arm type of symptom, I try to get them to narrow that down. Is their symptom interfering with activity? Is it interfering with sleep?
Patient Goal of Treatment
- Return to work
- Return to sport
- Perform ADL/specific activity
I want to know their goal of treatment. Is it to return to work? Is it to be able to do all of their activities at work? Maybe they are not able to do a certain task, but are they able to do others? Do they want to return to a sport or another specific activity? In the end, it is not about our goals and increasing motion, decreasing edema, or healing, or anything like that. It is really about their being able to go back to their daily activities.
- Complete once you understand the impact this condition has on the patient
- Psychologically
- Physically
- Socially
- Economically
Once you understand the impact of the condition on the client in all these areas, then the history is complete. You now know who this patient is. You now know why they are there. And, you now know what they want to go back to doing and what their goals are. As OTs, we know how critical the whole person and this whole picture is. Now, we are going to get into some specific tools that you may want to use and some specific areas that you are going to want to assess.
Pain
- Pain Reports: Intensity
- Verbal analog scale: 0-10
- Least/worst rating
- Duration, frequency, consistency
- Location
- Exacerbating/alleviating factors
Pain is a standard assessment that everybody does, whether you are a Joint Commission facility, a CARR facility, or anything that is billing insurance. Unless you are private pay, you need to complete some type of objective pain report. The primary one the majority of hand or upper extremity rehab therapists are using is some type of intensity scale. An intensity scale asks, "How bad is your pain?" Or, "Rate your pain." This is something that we constantly ask. We ask it at the beginning, during, at the end of treatment. There are many tools out there that you can use. I want to cover what types there are and make sure that you find one in the clinic that works best for your population and for you.
There is a verbal analog scale of zero to 10. There is also a visual analog scale, zero to 10. Typically, these are rated as zero or no pain. The 10 rating has two different definitions that most people apply to it. It can either be the worst pain that you have ever experienced or the worst pain that you can imagine. Those are actually two different things. If you think about it, I could imagine horrendous pain. Have I experienced a 10? Absolutely. So, you have to define that and make sure you are using the same language. Everybody in the clinic should have the same language that they are using for their zero to 10 scale.
There are both "least" and "worst" ratings. Tell me when you have your least pain. Tell me when you have your worst pain. You want to understand the duration, frequency, and consistency of their pain. Does their pain come and go? Does it stay all of the time? What is the location? What makes it worse? What makes it better? Those things are really important. Is there something that they can do to make their pain better? And, is there something that they do every day that makes it worse? Start to define that so that you can help them address their pain.
- Pain Charts
- Visual analog scale (VAS)
- Wong-Baker Faces scale
- Observational pain rating
- Pain drawings
There are also some visual components you can give them to fill out prior to coming back and seeing you.
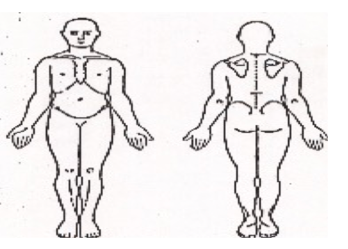
Figure 1. Pain scale drawing.
Pain charts such as a pain drawing can be used. There are observational pain ratings. There is also something called the Wong-Baker FACES that we use with the pediatric population. It is specifically normed for ages three to seven. It can also be used for people who are nonverbal or for some people who have cognitive delays. They may not be as accurate with giving their pain rating intensity, but you can show them the FACES, and they can rate their pain using those images. Make sure that the scale that you are using is correct for your client. The numeric rating scale has been reliably tested for ages 18 and up. If you use that with children, you need to be aware of that. There are also infant pain scales. There is something called the FLACC, which is for infants two months and up to about the age of three. This is an observational pain scale where you would watch the baby for things like how their extremities are moving and if they are consolable. There are pain scales out there for every population.
- What Makes Pain Better?
- Rest
- Ice
- Position
- Medication
