Teresa: Today we are going to talk about infants and young children, focusing on the early intervention population but up to about three or four years of age. I want to point out that I am going to be using terms of both parent and caregiver throughout the course and regard them as interchangeable, just as an acknowledgment to the many family configurations that we observe in our practice today. If the term mother is used, it is because that is how it is presented or reflected in the cited research.
What is Co-Regulation Versus Self-Regulation?
What is co-regulation versus self-regulation? And what does the literature have to say about those two terms?
Co-Regulation
It is rather difficult to find solid definitions of co-regulation. This one I found in Wikipedia says it is the "continuous unfolding of individual action that is susceptible to being continuously modified by the continuously changing actions of the partner." This can be co-regulation with a parent or a family member. Co-regulation may also be with another trusted person or loved one in the room. But as the child's therapist, you may also be called upon to be a co-regulator, and you sometimes see co-regulation being attempted, though often with failed results, with a family pet. What I got out of that definition, other than the overemphasis of it being continuous, is that the regulation is modified or modulated by the actions of a partner versus something that I would do on my own. And in my work, I use a much friendlier definition. "Co-regulation is to borrow regulation off of someone else's regulated body." That is the child in the room in interacting with you or the co-regulation partner is borrowing your regulation. This is something that speaks to families and lay people much more succinctly.
Self-Regulation
Self-regulation is a little more understood. There are many definitions that you can find out there about self-regulation. This is one of my favorite by Cook and Cook in their work in 2009. "Self-regulation is the ability to monitor and control our own behavior, emotions, or thoughts, altering them in accordance with the demands of the situation. It includes the abilities to inhibit first responses, to resist interference from irrelevant stimulation, and to persist on relevant tasks even when we don't enjoy them." We are matching our bodies to the environment or task. This is one of the important key concepts we see in self-regulation, as well as in inhibition, filtering, and what I would call task persistence, or what some authors have called grit.
Progression of Regulation
Let's talk about the progression of regulation through the lifespan. And though this is depicted as stairs, I want you to think of it like running up a sand dune (Figure 1).
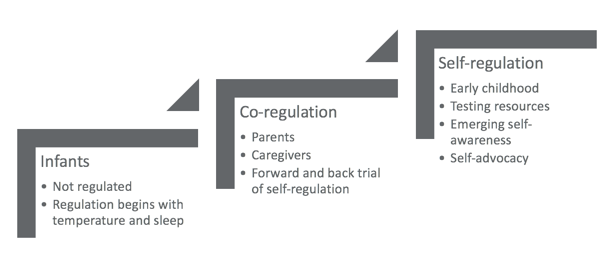
Figure 1. Progression of regulation through the lifespan.
We take some steps forward, but sometimes we slide back to more fluent and reliable lower levels of functioning. That is we can have some self-regulation even as we continue to co-regulate with others. It should not be perceived or understood that once self-regulation is "achieved" that we give up on co-regulation. We simply have more tools available once we can self-regulate than we do if we are restricted developmentally to our highest level being co-regulation with our caregivers.
As we know, infants are not regulated individuals. We see regulation begin to emerge in the typically developing infant with internal body temperature and sleep. From there, co-regulation begins to appear with parents or caregivers. And as that child develops in the twos and threes, you see a forward and backward progression of self-regulation. Sometimes it may be successful and sometimes it may not be. Then, the self-regulation you see emerging in early childhood, usually before a child begins school, is where that child is beginning to test their resources. They may have some emerging self-awareness of their ability to handle their own body and are beginning to explore self-advocacy.
Figure 2 is my own graphic that I designed to visually depict the dynamics of a successful co-regulation event.
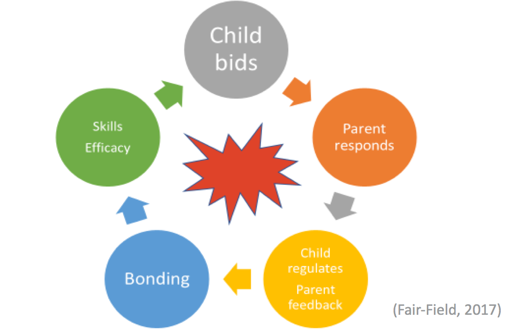
Figure 2. Successful co-regulation event.
It begins with an upset, which I have demonstrated by the red explosion. This is because with young children this is what it feels like. Explosions are how parents sometimes describe the event. So, an explosion happens and then the child makes a bid for co-regulation, which is shown as the gray circle. It is outside of the child's ability to self-regulate at their current stage of development. The bid can look a variety of ways. If it is successful, regardless of how the child presents the bid, the parent or caregiver will then respond with their own regulated body (the orange circle). As we have already described, the child will then borrow that caregiver's regulation and begin to regulate him or herself. The caregiver then receives some feedback by observing that the child is successfully regulating as shown as the yellow circle. We define success as the child becoming regulated in response to the caregiver and the caregiver being able to meet the child's needs. A bonding event is formed which is that cozy blue circle. Their relationship is then strengthened by that co-regulation event that was successful. And as we progress around that figure to its finish, we see in the green circle that the pair, the dyad of them, has developed skills in efficacy. This is by both the child who has learned something about what to do to regulate their own body, which contributes to the development of later self-regulation and then the parent who has learned what it takes to successfully support the child. This is shown as a continuous loop because those skills and efficacy then directly impact that child's next bid for regulation when another explosion comes up.
Differentiating Typical
One of the biggest challenges, particularly in articulating expected versus unexpected development relative to regulation, is what I hear parents so often comment, "Isn't this just the terrible twos?" The answer to that is "yes and no." Every child struggles with developing self-regulation at this age. This is the work of being two and three. However, some struggle more than others and are resistant to intervention or support. Or, they might linger in co-regulation well beyond when we would expect them to be developing some emerging self-regulation. What are those differentiations between a child with a challenging system? How can we articulate these characteristics to parents and caregivers?
- Able to participate in a group with similarly aged peers.
- Can join play in progress?
- Able to adjust behavior to cues.
- Able to lead or follow.
- Collects information from the environment.
- Changes gears relatively easily.
- Recovers relatively quickly.
- Struggles to join or remain in a group.
- Disrupts play in progress.
- Struggles to turn off a behavior, even when prompted.
- Appears to be on his/her own plan, or only lead the action.
- Upset when having to change gears (i.e. ‘transition’)
- Takes a long time to recover.
Looking at typical, we see that the child is able to participate in a group with similar age peers. They may struggle to join or remain in a group. We see this so commonly hand in hand with the next item, which is a child with typical self-regulation can join, play, and progress. A child that is struggling with that will disrupt the play and progress when they attempt to join. Typical self-regulation is the ability to adjust behavior to cues. The typically developing two- or three-year-old may not inherently respond with the right behavior, but they can adjust it to the caregiver's cues; whereas, if they are struggling with regulation, they will have difficulty turning off a behavior even when it is prompted. With typical self-regulation, you see a child that is able to be in either a leading or following role. In contrast, some children appear to be on their own plan or insist upon leading the action in order to be successful. With typical self-regulation, you see a child that is collecting information from the environment and then uses that information to change gears relatively easily. And if they are struggling, they are upset when they have to change gears, what we so often refer to as a transition. Rather than recovering relatively quickly, they tend to take a long time to recover and can be quite disruptive to the family system.
Factors Affecting Regulation
What are some of those factors that lead to disordered regulation? It is a long and confounding list.
- Genetics
- Environment
- Neurological development
- Adverse Childhood Experiences (ACEs)
- Intrauterine Exposures
- Prematurity
- Allergies/Digestion/Physical Symptomatology
- System maturation
- Accommodation/Strategy/Exposure
Genetics (nature) and environment (nurture) are some of the factors. This is going beyond the home environment and looking at all of the sensory environments and experiences the child might be routinely exposed to. You see neurological development, as well as adverse childhood experiences, what we call ACEs as other factors. We will be discussing these more as they significantly impact co-regulation and bonding, which later affects self-regulation, even in otherwise typically developing children. Intrauterine exposures, prematurity of any amount, allergies, digestion, physical symptomatology, that may be causing discomfort, and maturation of the nervous system are some other factors. Finally, accommodation strategy and exposure provided by caregivers rounds out this list. With so many confounding factors affecting regulation, it can be difficult to sleuth out which is the cause. Some of the items on this list are modifiable, particularly when we look at physical discomfort. We need to address this concurrently with therapy, but some are historical. Making the best recourse for the practicing therapist to address the child and family system, as they currently present, is what we are going to be looking at as they appear in the literature.
Indicators of Poor Regulation
Many authors have described these conditions and in great detail. I am presenting them here as talking points to use when you are speaking with parents. Often in early intervention, children are arriving in our caseload without having a formalized diagnosis of any kind. And so, we need to speak to those caregivers in more functional terms. Figure 3 shows these layperson-friendly terms.
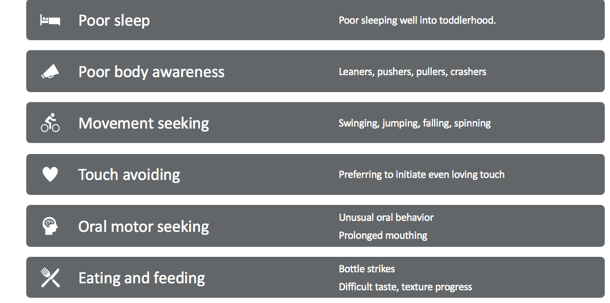
Figure 3. Layperson-friendly terms.
One indicator of poor regulation is poor sleep well into toddlerhood. While we expect some difficulty and challenge with early sleep if sleep is not resolving this can be an indication of poor regulation or difficulty emerging self-regulation. Poor body awareness can be seen in our leaners, pushers, pullers, and crashers. Movement seekers are swinging, jumping, falling, spinning, and doing other vestibular activities. Touch avoiders are those children that prefer to initiate even loving or friendly touch. Those that are oral motor seeking have unusual oral behavior or prolonged mouthing. Finally, eating and feeding issues that can be seen with bottle strikes as well as challenges with taste and texture progression.
ACEs and (Co-)Regulation: Effects of Early Childhood Experiences
Let's focus on ACEs in co-regulation and what the effects of those early childhood experiences are.
Adverse Childhood Experiences (ACEs)
- Personal experience of abuse, neglect, trauma
- Proximity to an unstable parent or close family member (substance abuse, mental illness, domestic violence)
- The sudden departure of a close family member (divorce, death, incarceration, abandonment)
Adverse childhood experiences can be personal experiences of abuse, neglect, trauma, or proximity to an unstable parent or close family member, including those with issues of substance abuse, mental illness, or domestic violence. It would also include the sudden departure of a close family member, such as through divorce, death, incarceration, or abandonment. There are many resources available online to begin researching the effects of ACEs, not just to the pediatric client but throughout the lifespan. And, you can begin to expect to see more and more evidence of the latent effect of ACEs on the development of the nervous system. In the scope of this course, we are going to be discussing how bonding and attaching affect regulation, and how the experiences of ACEs impact that process.
Disrupted Neurodevelopment (Lynch, Ashcraft, & Tekell, 2017)
- Impedes typical maturation of the CNS
- Difficulties with discrimination, praxis, and modulation
- Layered upon ‘at risk’ systems due to pre-natal/intrauterine exposures
Multiple citations in the literature of the ACEs pyramid begin with disrupted neural development and culminates in chronic disease and early death. The experience of ACEs after a certain point or a certain collection of events impedes typical maturation of the nervous system. The child's experiences actually begin to affect their neurology. We see difficulties with discrimination, praxis, and modulation. This is layered upon systems that are considered at risk due to what is possibly an already exposed child to prenatal or intrauterine exposures that often go hand in hand with those ACEs experiences.
Relationship Between Attachment and Sensory Modulation
Whitcomb, Carrasco, Neuman, and Kloos (2015) looked at connecting sensory modulation and attachment or bonding. What we saw in my figure earlier was how self-regulation is developed via a secure attachment. Sensory modulation is a bit of an older term and has been somewhat replaced by the term sensory reactivity. Modulation describes the nervous system's ability to accommodate input and then determine an appropriate output so sensory modulation is still very commonly seen in the literature. It is an important component of regulation and one that particularly concerns us as occupational therapists. The Whitcomb et al. study included:
- Statistically significant
- 68 Children ages 3-6 with the primary caregiver for 12 m
- Excluded children receiving tx for either concern
- Attachment Q Set & Short Sensory Profile
- Natural environment session of 60-75 min
Whitcomb, D. A., Carrasco, R. C., Neuman, A., & Kloos, H. (2015). Correlational Research to Examine the Relation Between Attachment and Sensory Modulation in Young Children. American Journal of Occupational Therapy, 69(4), 1–8.
This research team looked at 68 children, ages three to six, that was with a primary caregiver for 12 months. This was not necessarily a parent or family member. It did exclude children receiving treatment for either attachment or sensory modulation. They were evaluated using the attachment Q set, which is a psychological assessment tool, as well as Winnie Dunn's Short Sensory Profile. They also observed in a natural environment session of 60 to 75 minutes. Their work focused on three research questions:
- Is there a relationship between attachment and sensory modulation?
- Is the health of the attachment relationship predictive of their sensory modulation function?
- Is sensory modulation function predictive of the health of the attachment relationship?
They found that both young children, who are insecurely attached, may struggle with correctly interpreting and responding to sensory stimulation from the environment. And, children, who initially have atypical responses to sensory information, may have difficulty forming a healthy attachment to their primary caregivers. So, both attachment and sensory modulation can both explain and predict the other. For example, if the child is highly reactive, the caregiver may become less competent and more tentative in their responses, resulting in less consistent and less frequent engagement with the child, or even withdrawal. And then, of course, we know that if caregivers are distant or unresponsive, children develop insecure attachment, which may limit their exposure and exploration. Reduced exposure then impacts their ability to adapt.
Sensory behaviors as a coping mechanism:
- poor adaptation skills
- sensory reactions trigger emotional states
- emotional states trigger sensory reactions
- perceived loss of control (remember volitional impact)
One thing that has been observed as a result of this study is that sensory behaviors in this population can perform as a coping mechanism. The child has poor adaptation skills and the sensory reactions tend to get co-mingled with emotional states so that one triggers the other, and it happens in both directions. So sensory reactions are triggering emotional ones and emotional ones are triggering sensory ones. We also see in the ACE's population a perceived loss of control. If we remember the impact of volition on the nervous system, that will help us understand this a little bit better to explain this to parents. If the child has control over the input and can gate the input themselves, it is perceived better by the nervous system than if the input is thrust upon them from the environment.
