Barbara: It is good to be here today. I want to give you a little background about why I am doing this presentation. I have recently been running a return to work program for the United Spinal Association. I have been working with people with spinal cord injuries who want to go back to work. One of the things that was startling to me was that no one in rehab talked to them about going back to work. As occupational therapists, we probably spend more one-on-one time with our clients than any other profession. PT does a great job, but they are not working one-on-one for the most part. We have a lot that we can be doing during that time. Today, I want to look at how we can infuse work into the conversation and into what we do.
Work
The Occupational Therapy Practice Framework (OTPF) explains several aspects of "work".
Page S11 in the Framework: “Occupational therapy practitioners also provide consultation to community organizations such as park districts and civic organizations that may or may not include people with disabilities. In addition, practitioners consult with businesses regarding the work environment, ergonomic modifications, and compliance with the Americans With Disabilities Act of 1990 (Pub. L. 101–336).”
First, it talks about occupational therapy practitioners consulting with other organizations to comply with the ADA, like parks and recreation or Meals on Wheels. It also talks about helping businesses comply with the ADA with ergonomic changes or employee accommodations. Many OTs think this is a specialty area. I ran work hardening clinic in the late 90's and early 2000's, before autism was so popular and ubiquitous. During this time, I did a presentation on playground accessibility under the ADA in Texas, and some OTs came up to me during a break and said, "We are being asked to do psych OT." I thought, "What does that mean?" They said that they were being asked to treat kids with autism. As I happen to have two children (now adults) on the autism spectrum, I chuckled in side. I said, "Do you treat kids with ADHD and sensory integration issues?" They replied yes. I said well what you do with them is pretty much the same thing. They have sensory issues, they may have motor coordination issues, and there are also some social skills components. Along the same lines, I do not consider myself a "work OT" or a "peds OT". Not everyone is going to be an expert. But when you go to the park, if there are steps to get to a certain place at the park, it is not accessible and we can offer an alternative. Conversely, if we have a client who wants to go back to work, we can help them problem solve, because that is our big skill. We have a set of tools that allows us to look at a situation and say, "How can this be different? How can we change it? How can we make it usable?"
“Labor or exertion; to make, construct, manufacture, form, fashion, or shape objects; to organize, plan, or evaluate services or processes of living or governing; committed occupations that are performed with or without financial reward” (Christiansen & Townsend, 2010, p.423).
This might be volunteer work or paid employment. It is looking at how people create things. This involves task analysis. We look at how things are made, we look at the steps, and we look at how we can intervene in the steps and enable people to perform. Do we need to change the task, change the person, or do we need to change the environment? It all goes back to basic occupational therapy. This is what we do. Another section of the framework talks about employment interests and pursuits which is identifying and selecting work opportunities based on the individual's characteristics; what they like, what they do not like, and what their limitations are (Adapted from Mosey, 1986, p. 342). During OT intervention, we look at people's limitations, their strengths, their likes, their dislikes and we pick tasks for them to do.
Work and the Framework
The next section of the framework that was relevant was employment seeking and acquisition. A big part of this is advocating for oneself. What do people need to know to advocate for themselves? I am going to teach you where to find resources looking at materials and interviews, but also looking at policies and benefits. There are a lot of benefits out there that are designed to help people go back to work without losing all of their benefits. There are also work incentive programs. I do not expect you to be an expert in them as that is not the purpose of this presentation, but is to know that they are there. By knowing these resources, we can steer our clients in the right direction. We will also talk about job interviews because having a job interview after a disability is very scary.
We also look at job performance. This looks at work skills and patterns, time management, and getting along in the workplace. We are going to talk about autism as an example, because we see so many people with autism transitioning to adulthood who do not know how to act or socialize in the workplace. They need to know how to maintain a job and understand what the norms are, or how you are supposed to act in the workplace.
Reimbursement Practicalities
There are some practicalities when it comes to reimbursement because we know that health insurance pays for medically necessary occupational therapy intervention. Most health insurance very specifically excludes payment for what they consider vocationally relevant intervention. Workers compensation will pay for it, but when we have a rehab patient or a patient in acute care, they are not covered by workers compensation; they are covered by health insurance. The question becomes, how do we pay for this? And, are we doing anything special or different that needs to be looked at as something that takes things it out of being medically necessary and moves them over into the vocationally relevant column. What I am asserting is that the work discussion is a discussion. Often, you become an integral part of their family or households, especially when you treat them for an extended period of time. You get to know a lot of intimate details about their lives. Can we use this time to incorporate work activities into their intervention? We know that work activities and functional activities can increase range of motion, muscle strength and coordination. Instead of talking about Aunt Mary or so-and-so's wedding, the discussion can be work related. Have you thought about going back to work? What are your plans now? What are your concerns about not being able to work again? What do you think might be a barrier? How can we change some of these things? Make that discussion geared towards work so that we are using our time efficiently to make people feel more comfortable about their path to return to work and successful employment. As I said, we spend more time with our patients than any team member. We can direct that discussion towards work, or plant the seeds to move people down that path to work or towards transition (for kids and teens).
Our Life Roles
I want to talk a little bit about our roles, as seen in Figure 1.
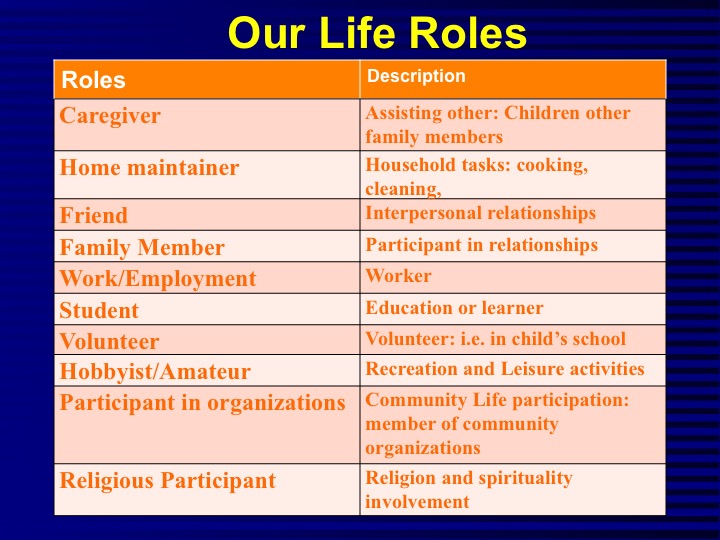
Figure 1. Life roles.
We can have many roles like caregiver, home maintainer, friend, family member, worker, student, volunteer, hobbyist, etc. The one I want to point out is the worker role. When you are/were in college, people always ask, "What is your major?" When you are an adult, they ask you, "What do you do?"
The Worker Role
Work is a very significant part of people's lives, and it is part of their identity and who they are. When you take that away, it changes people and what their roles in life are. Fisher, 1999, says that being a successful worker is dependent on your capabilities, your habits, your every day routines, your interests, and your motivation. Mentoring can help people explore those capabilities, habits and every day routines, and reinforce their interest and motivation to work. I see our role as a mentoring role. We are being supportive and being a coach for our patients. As the capacity to work and the interest and motivation increase, we can talk about successful experiences and successful ways to return to work, what steps they can take, and determine the barriers are and ways to eliminate those. Learning about successful pathways to employment can help people change their habits and routines to match those needed for their own pathway to employment.
I am now going to give you a series of case studies that look at how can we put work back into occupational therapy practice. These are based on real things that have happened.
Case Study #1
Dr. B is a 55-year-old surgeon who is recovering from Guillain-Barré syndrome. For those of you who are not familiar with Guillain-Barré syndrome, it is a condition that people get following a vaccine, virus, or some illness. They often are paralyzed. They get motor return; typically the intrinsic muscles of the hand return last. Often they use plasmapheresis, or plasma exchange, to treat this. He came to occupational therapy and he did not really see much in the department that interested him. He was very worried that he was never going to be able to perform surgery again and was not sure why he was in occupational therapy to begin with. Due the Guillain-Barré, he had weak intrinsic muscles. What about work simulation? You are probably wondering how can you simulate surgery in an occupational therapy clinic. We were able to do this by having him "operate" on vegetables. That may sound kind of crazy, but we got a suture kit and vegetables. He had to take the seeds out with tweezers. He had to suture the tomatoes back up again with the suture kit. He was very happy. He felt that he was working on skills that he needed to return to surgery. This was not someone who would have been happy doing anything else but simulating his work. At first he kind of laughed, and then when he started operating and trying to suture a tomato, he said, "This is harder than suturing people." It changed his whole attitude when he was doing work activities. We need to be creative instead of having clients do the same activities over and over.
Case Study #2
SW is a 62-year-old office manager in a large insurance company. She had a relatively mild right CVA and has been out of work for eight weeks. She would like to return to work but is a little scared about that. She does not know if she is going to be accepted back to work. There are so many questions that this raises. At 62 she has a long life ahead of her and is not ready or willing to just retire and get disability benefits. First of all, there is the Family Medical Leave Act.
Family Medical Leave Act
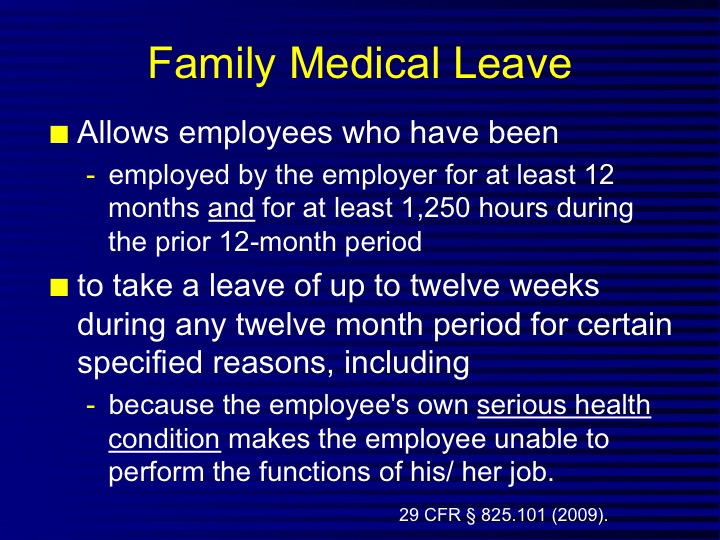
Figure 2. Overview of the Family Medical Leave Act.
As long as the employee has been employed for 12 months and have worked at least 1250 hours during those 12 months, they can take a leave up to 12 weeks during any 12-month period for many different reasons. One that is relevant here is a serious health condition. The health condition has to make the employee unable to perform the functions of his or her job, which certainly having a stroke did. She was not able to perform her job. They cannot NOT take her back because she took this leave. She had to follow the company's procedures for taking the leave, and that is one of the things she did. You can also have a family member to request the leave.
After the family medical leave was over, Selma was concerned that she would not be able to type on the computer with both hands since her involved hand had limited range of motion and coordination. This is a conversation that we need to have while we are working one-on-one with Selma. In addition to safety and environmental accommodations for home, we can also address these work issues.
ADA Reasonable Accommodations
The ADA provides for reasonable accommodations in the workplace (see Figure 3).
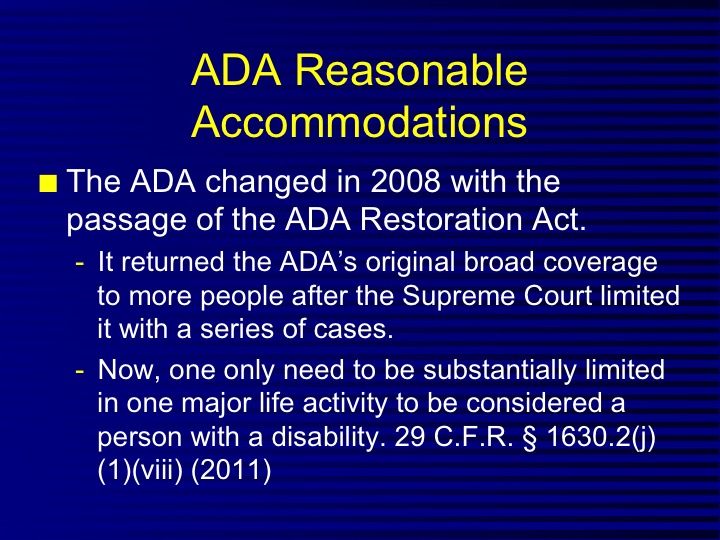
Figure 3. Overview of ADA and reasonable accommodations.
This all changed in 2008. I am not going to go into a whole lot of detail, but Congress passed the ADA Restoration Act because the Supreme Court had limited the ADA with a bunch of cases that it decided in one day. It said that you had to be limited in more than one major life activity. Congress said, "No." You only need to be substantially limited in one major life activity to be considered a person with a disability. Congress wanted this broadly interpreted.
The new definition of disability is a physical or mental impairment that substantially limits a major life activity, or record of such an impairment, or being regarded as having impairment. I am not going to go into the regarding paragraph here because we are really only talking about the first two, which is having a physical or mental impairment that substantially limits a major life activity or having record of such impairment. We know that Selma has impairment. The major life activities that they define in the law were expanded to include things like caring for oneself.
Major Life Activities
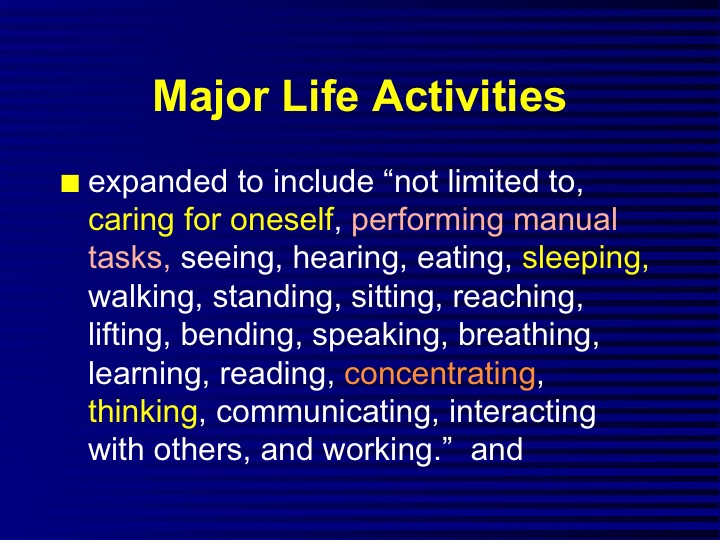
Figure 4. Definition of major life activities.
Selma has some weakness so she may have difficulty dressing and bathing, which would be caring for herself. Performing a manual task is another one that she has difficulty with because she has right side weakness and she cannot use the typewriter with both hands. She does not have issues with seeing or hearing. She may have some eating problems. Some other areas of concern are: concentrating, thinking, interacting with others and working. She would be substantially limited in doing her job.
Major Bodily Functions
The major bodily functions are outlined in Figure 5.
Figure 5. Major bodily functions.
A stroke would come under the neurological system. If we were working with patients who have hand injuries for example, that would be musculoskeletal. If we are working with children, that would probably be again neurological if there is some developmental or sensory issues. This pretty much covers most of the people that we see. It will also consider an individual organ that is not working.
Preparing For Return To Work
Selma needs to prepare for work. Often, I give my clients this chart about transition (see Figure 6).
![]()
Figure 6. Transition chart.
Transition is a time for learning new information, developing skills, making decisions, and taking action. It all involves planning. What do I need to do to return to work? What steps do I need to take to do them? For Selma to return to work, she first needed to tell her boss that she wanted to come back to work. She also had to tell him the difficulty she was having using the computer. What reasonable accommodations could she use?
