Kathleen: Thank you so much for that introduction. I want to thank everyone who has come out this afternoon for our talk on sexuality in long term care. Before I jump into the information, I want to tell you that sexuality in long-term care is much greater than just in the microcosm of OT. We are going to lead off talking about a lot of general issues that you may see within the facility because the reality is you probably will be pulled into many of these issues regarding consent and policies. I want to lead with that background, and then we are going to talk about some very specific diseases and conditions that OT can address sexuality within.
Myth or Fact
- Older adults are not interested in or able to have enjoyable sex.
What do you think? This is a myth. Most older adults are in fact interested in sex. Many lead active sex lives and enjoy sexual activity; 87% of married men and 89% of married women in the age range of 60 to 64 are sexually active. In fact, 54% of sexually active older adults are having sex at least two to three times a month. Oral sex is reported by 58% of sexuality active people aged 57 to 64 and by 31% of those aged 75 to 85. Masturbation is reported by 52% of men, 25% of women who are in intimate relationships, and 55% of men and 23% of women who are not in relationships.
- Older adults do not have to worry about contracting sexually transmitted diseases like HIV or AIDS.
This is definitely a myth. Older adults who are having sex with people, other than life partners, do have to worry about sexually transmitted infections just as much as younger adults in the same situation. They should be practicing safe sex by either using a male or a female condom. There are about 75,000 individuals over the age of 50 in the U.S. that have been diagnosed with HIV or AIDS. This is about 10% of the total number of cases in the United States. Unfortunately for reasons that we will talk about in just a little bit, this number is on the rise.
- Continuing physical challenges keep seniors from having sex.
This is a myth. As you get older, sex may require some creativity, but it is still possible to compensate for many of the issues that adults have and to remain sexually active. It is actually very healthy. Unfortunately far too many people encounter an obstacle, such as low libido or erectile dysfunction, and they do not know who to talk to about it, and because of that, they just give up on sex all together. It is really important even from our perspective that we encourage them to discuss it with their physician.
- Seniors cannot avoid pain during intercourse.
This is also a myth. Women do experience biological changes that may result in uncomfortable or painful intercourse. For example, hormonal changes can cause vaginal tissues to become dryer, and there may be pain, as well as other types of pain from arthritic changes. They may require a change in position, additional pillows for support, or over the counter pain medication. We will be talking about different positions as we go along here.
- Sex is dangerous when you reach a certain age.
I think this is a funny one. Obviously that is a myth. Sex is unlikely to cause anything worse than aches and pains from unused muscles or arthritic joints. In fact, a lot of studies show that being sexually active can improve your mental, emotional, and physical health.
- Sexual problems are just part of normal aging without any solutions.
Of course that is stated in a way that makes it obviously a myth. There are a lot of issues that may exist, but many of these are treatable by the physicians. Some of them we can address in therapy. Again we need to encourage our folks to talk to their physicians because their physicians are trained to address issues of sexuality in an unbiased, empathic, and a nonjudgmental manner. That is actually where we want to get to as well, and we will be talking about that in just a moment.
Physical Changes in Women/Men
There are real changes in women and in men as we age that may in fact affect their sexual function.
- Lower libido or slowing of sexual arousal
- Hot flashes and/or night sweats
- Sleep disturbances
- Emotional changes
- Vaginal dryness and itching
- Increased sensitivity to sounds
- Dry skin
- Weight gain and/or food cravings
For women, they may see lower libido, slowing of sexual arousal, hot flashes, dry skin, vaginal dryness, and itchiness that sort of thing. With men, they may need a longer time to obtain an erection, have an inability to maintain it, and increased time between erections. Again, these are very normal changes, but unfortunately, these changes can be exacerbated either because of a disease, by medications, or some other thing that has happened.
Introduction
Definitions
Starting with sexuality, so there is a council called the Sexuality Information And Education Council in the United States. They have defined sexuality as a part of personality that encompasses sexual beliefs, attitudes, values, behavior, and knowledge. Beliefs, attitudes, values sound very similar to the OT Practice Framework and the Occupational Profile, thus, I think this is a natural collaboration with occupational therapists. One of the most important things that everyone can do regarding sexuality is to first uncover your own biases and figure out what your own beliefs are. As we look at what is appropriate and inappropriate behavior and also what we will or will not tolerate, this is guided by our lens of what we think is appropriate and what our values and attitudes are towards sexuality. It is really important to be able to uncover some of those biases.
Sexual intimacy is the interpersonal relationship between two people who may or not be engaging in sexual activity. The emphasis here is on the emotional experience and the feelings of closeness. We need to understand that sexuality is not just sexual acts or intercourse, but it is multi-dimensional and affection as well. Sexual expression can include things like kissing, fondling, masturbation, oral sex intercourse, touching, hugging and the like. Expressions can include things like sending flowers, maintaining beauty, flirtation, affection, and so on and so forth. If you look at this list in Figure 1, many of these things are considered to be inappropriate at our sites.
Figure 1. Sexual expression examples.
Again we have to step back and recognize that older individuals often define and express their sexuality in very different ways than younger persons. This suggests that there are changes in sexual expression that may occur with age.
Domains of Sexuality
There are three domains of sexuality, as shown in Figure 2.
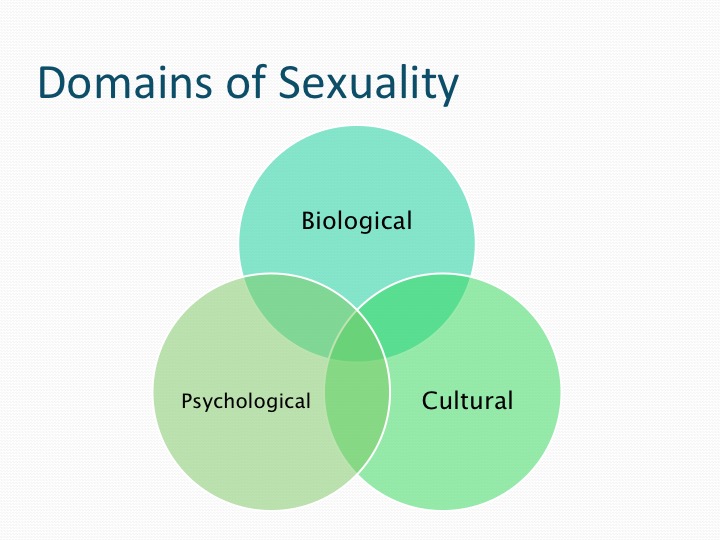
Figure 2. Domains of sexuality.
There is a biological domain, which are the inherited factors of being male or female, sexual differentiation, our hormones, our orientation, and our sexual health meaning whether or not we are free from disease. The psychological domain involves feelings or the emotional side of things and interpersonal relationships. Finally, the cultural side is the media, religion, sex education and everything that you read, see, or hear out in the environment. Overall the important thing to note is that our attitudes and overlay culture influence the domain the sexuality much more than anything that is biological.
AARP Study
Here are a few more numbers for you from an AARP study that was done back in 2010 (see Figure 3).
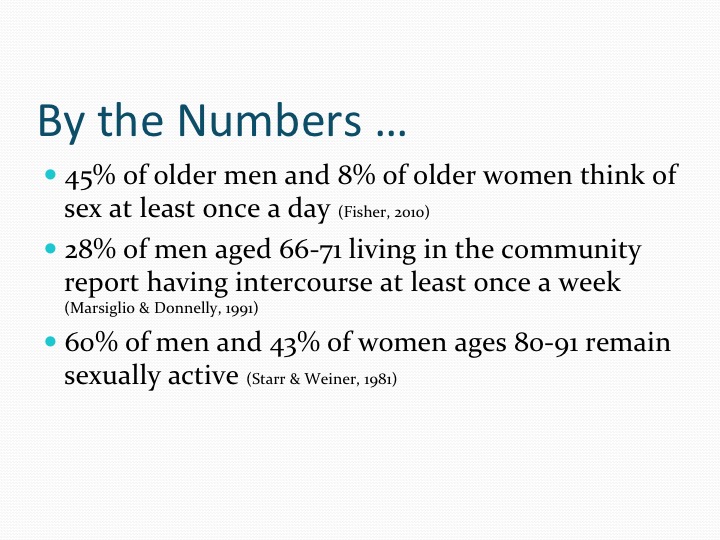
Figure 3. Stats from AARP.
It found that 45% of older men and 8% of older women think of sex at least once a day. Additionally, 28% of men, aged 66 to 71 and are living in the community, are having intercourse at least once a week. Finally, 60% of men and 43% of women ages 80 to 91 are still sexually active. We have to remember that even though there might be a decline in sexual function with age, the activity and the interest is still there well into old age. It may just take a different format.
Sexuality in Long-Term Care
When we look specifically at long term care, an interesting poll from the same AARP study indicated that 25% of people who are living in an SNF say they are always lonely and 40% say that they are sometimes lonely. To alleviate this, we need to promote intimate relationships. The big fear is that they are going to die alone, and they are looking for some closeness in an intimate relationship. Someone who can help to ease that transition and achieve a peaceful death. Again, this does not have to be a sexual relationship; it could be an intimate relationship. Remember that there is a big difference. The demographic is now starting to change a little bit in our facilities, but I think the folks who are in our facilities right now grew up at a time when sexual behavior really was not discussed. It was actually suppressed versus being encouraged and talked about. The education about sexuality was very minimal. If you think about the meaning behind sexuality, there were a lot of gender differences. Pleasurable sex was meant for men. While for women, sex was for procreation and to please their husband. Many individuals were taught that there was no sex prior to marriage, and have only had one sexual partner in their entire lifetime. This is also something interesting to consider. We are going to talk about more of this, but again intimacy and sexuality are not necessarily the same thing. Again, I find it interesting that these are folks have been sexual all their lives, but as soon as they walk into long term care facility, they need to check it at the door. Older adults are encouraged to be asexual. They are often labeled as behavior issues. We, as OTs, can encourage other ways to address that intimate need; hair grooming, hand massage, or even just having consistent staffing so that a resident can to talk to the same person and develop a relationship.
Staff Attitudes About Resident Sexuality
Let's talk about staff attitudes about residents' sexuality, starting with what I call the ick response. Was there ever a time that you caught your parents having sex and you told your friends about it? What was the response? They probably rolled their eyes with horror. Often in long-term care, we have the exact same type of response to our residents. We cannot believe it, and we are shocked.
Sexual Expression in LTC
There are three types of sexual expression that we see in long term care. The first is love and caring, or a strong affection between two residents. That may progress to romance where someone is the object of someone else's affection. Eroticism is that next level where we have feelings of sexual excitement or desire that may result in intercourse or some sort of sexual behavior. Generally speaking caregivers are really sympathetic toward love and caring. We find these relationships cute. We think they are endearing. We liken them to the first time we fell in love. It is cute unless it leads to something more involved or something sexual. If it does lead to something more involved, oftentimes we frown upon that. We separate people. We move them out of the facility. We label them as behavior issues. We oftentimes will encourage a relationship providing it does not go too far.
Staff Responses to Sexuality
In 2004, Roach identified four different staff responses to sexuality. Some of these you may have seen or are familiar with. The first is called standing guard. We address sexuality in a way that makes us feel less uncomfortable than any other situation. We avoid dealing with the situation. If a new relationship starts, we separate the residents before it goes any further, but this is likened to cause decrease quality of life, depression, and poor satisfaction. The next type of response is reactive protection where we also avoid staff uneasiness. We treat the residents as if they were children. It is very paternalistic, and we encourage them to refrain from sexual activity. Next is something called guarding the guards. This is where staff comes up with ways to implement an approach to sexuality in that restrictive environment. We know that there is a forbidden relationship, but we do what we can do kind of behind the scenes to encourage it. We have this drama and secrecy. To everybody involved it is kind of fun and exciting, but it is definitely not the best approach. The best approach is something called proactive protection where we train and educate staff about sexuality, as well as a way, to respond to a client's needs in a dignified, respectful, and consistent way. We have a lot of positive outcomes here. OT can play a great role in this proactive protection response. We can teach the nursing staff, physicians, and even family members that sexuality is normal as we age.
Inappropriate Responses
There are many inappropriate responses to sexuality.
- Placing notes on the medical record
- Reporting sexuality at meetings
- Snickering or giggling
- Discussing sexuality with colleagues
- Reprimanding or otherwise scolding
- Praying over the person
- Invasion of privacy
Notes can be placed in the medical record. For example, so and so was masturbating, or somebody was reading pornography. People snicker or giggle about it, and it is reported at the team meeting. I am not saying that we should not report on certain things if they are a safety or an ethical concern, but we also need to consider privacy. You have to consider if you were having an intimate relationship would you want somebody reporting on it at your Home Owner's Association meeting? We want to treat it the same way and not report unless we absolutely have to. I have worked in some religious facilities where I have seen somebody come in with a bible and pray over a person due to masturbating or sexual orientation.
SAID Survey (Kunn 2002)
Kuhn in 2002 came up with something called the SAID survey. It is regarding staff attitudes about intimacy and dementia. While it is reflective of our attitudes about sex as it relates to dementia, I think it goes even further than that. I provided it as one of your handouts. It helps us to determine what our own biases are, what our stereotypes are, and what our opinions are. There is no right or wrong answer to these survey questions. It helps us to figure out where we need additional training. As OTs, we have a huge opportunity to provide education to our facilities in these areas. Some of the questions are on the slides. I am not going to read all of them to you. An example is: Competent and consenting residents who are single are entitled to be sexual intimate.
