Cara: I am currently in school for my doctorate in occupational therapy. I am excited to be here talking about some things that I have learned to complement the course. I have always been interested in Down Syndrome as a pediatric therapist. I have been a therapist for 20 years, and it is always interesting to learn more about a topic. Down Syndrome is something that we are all aware of because it is one of the most well-known special needs population that we care for as therapists. We are going to take this next hour to delve into what makes people with Down Syndrome really special and wonderful. And, we will look at what we can do as therapists to support their growth and development throughout the lifespan.
My sixth book is due out today, and it is called "Interoception." I am excited about it because it talks about how we feel on the inside. We are going to talk about some of that today to see how we can help those with Down Syndrome to interpret how they feel with emotions and sensory perceptions.
My own children are both on the autism spectrum. They are 15 and 18 years old. I do know what it is like to live and work with young adults with special needs. As a result, I am quite passionate about working with kids and helping them to have the most functional life possible.
What is Down Syndrome?
I do not like slides with a ton of information, but I have put this in there so you have the information later.
“In every cell in the human body, there is a nucleus, where genetic material is stored in genes. Genes carry the codes responsible for all of our inherited traits and are grouped along rod-like structures called chromosomes. Typically, the nucleus of each cell contains 23 pairs of chromosomes, half of which are inherited from each parent. Down syndrome occurs when an individual has a full or partial extra copy of chromosome 21.”
“This additional genetic material alters the course of development and causes the characteristics associated with Down syndrome. A few of the common physical traits of Down syndrome are low muscle tone, small stature, an upward slant to the eyes, and a single deep crease across the center of the palm – although each person with Down syndrome is a unique individual and may possess these characteristics to different degrees, or not at all.”
https://www.ndss.org/about-down-syndromeown-syndrome/
Our body is made up of cells, and each cell contains 23 pairs of chromosomes. Mom gives half and the dad gives half. There are 23 pairs which make the child a unique individual. Down Syndrome is a result of a partial or full extra chromosome 21. Another name for the disorder is called Trisomy 21, which means an extra or three copies of chromosome 21. This little piece of genetic material changes in everything in the baby. It changes physical characteristics and many predetermined things. I encourage you after this course to go and research a little bit more into what each chromosome has as there are different sections of chromosomes. There are also many genetic disorders that comes along that specific part of the chromosome.
Important Things to Remember
- Down vs. Down’s syndrome
- Down syndrome is named for the English physician John Langdon Down, who characterized the condition, but did not have it.
- While Down syndrome is listed in many dictionaries with both popular spellings (with or without an apostrophe s), the preferred usage in the United States is Down syndrome. The AP Stylebook recommends using “Down syndrome,” as well.
- ALWAYS use person-first language
- The word ‘retarded’ is NEVER appropriate!
- Use new and accepted terminology such as intellectual or cognitive disability
A few of the common physical traits that we see are low muscle tone, small stature, eyes that tend to slant upwards, and there can be a single deep crease across the center of the palm. Like any other disorder, there can be variances from the mean.
An English physician John Langdon Down is the one that characterized the condition. That is why it is called Down Syndrome. You should not use the term Down's child. You are not using person-first language. Keep that in mind as you are working with or documenting about children or adults with Down Syndrome.
The word mental retardation or retarded is also not appropriate. They changed it to intellectual or cognitive disability. You can look at your APA handbook, which is the handbook that classifies different disorders.
Down Syndrome Fast Facts
- The most common chromosomal condition diagnosed in America.
- 6,000 babies are born each year
- According to the Centers for Disease Control, Down syndrome occurs in about 1 out of every 700 babies. (Parker et al., 2010)
- Usually caused by an error in cell division called nondisjunction
- Occurs at conception and NOT related to actions of the mother.
- 80% of children with Down syndrome are born to women under 35 years of age
- Life expectancy for people with Down syndrome has increased dramatically in recent decades – from 25 in 1983 to 60 today.
(National Down Syndrome Society, 2017)
Down syndrome is the most common chromosomal condition in America. I did not include statistics from other countries, because most of us are in America, but I encourage you to look at statistics from your country. The Centers for Disease Control (CDC) completed a study in 2010 which stated that 6,000 babies are born each year, and that is the one out of every 700. It is pretty common.
We know that the error is in the cell division, but it is specifically called nondisjunction. We will talk about that more in a few slides. Parents that have children with special needs, and I am one of these parents, tend to blame themselves. There is a huge rate of divorce in families with children with special needs. We need to encourage parents that no one is to blame. Approximately 80% of these kids are born to women under 35 years of age, not to older parents as many believe.
The life expectancy for those with Down syndrome in 1983 was really low at 25 years old. The life expectancy today is 60 years old. Of course, we would like these families to have their family members even longer. We are going to work on that over the next 30 years.
About Chromosome 21
- The smallest human chromosome, spanning about 48 million base pairs (the building blocks of DNA)
- It represents 1.5 to 2 percent of the total DNA in cells
- Was the second human chromosome to be fully sequenced
- According to Scientific American: “Down syndrome is associated with more than 80 physical and mental problems, including congenital heart disease, an increased risk for certain leukemias, and immunological deficiencies.”
Chromosome 21 is the smallest human chromosome. That is interesting considering it is so impactful. There are 48 million of these base pairs, and it is only 1.5 to 2% of the total DNA in our cells. It is also the second human chromosome to be fully sequenced.
The Scientific American is a great source, and they say that Down syndrome is associated with more than 80 physical and mental problems, among them are congenital heart diseases, an increased risk for certain leukemias, and several immunological deficiencies. They know that because there are also some building blocks that reside on that same chromosome.
- Mutations in 14 known genes on chromosome 21 play roles in one form of Alzheimer's disease, amyotrophic lateral sclerosis, and progressive myoclonus epilepsy, among other diseases.
- Also on chromosome 21 are genes that are as yet unidentified, but known to be responsible for five so-called monogenic disorders, including two forms of deafness and Usher and Knobloch's syndromes.
The mutation is in 14 known genes on this specific chromosome. They play roles in one form of Alzheimer's disease, amyotrophic lateral sclerosis (ALS), and progressive myoclonus epilepsy, among other diseases. There are also unidentified genes that scientists that are not yet identified. They are suspecting at this point that there are two forms of deafness, and they are looking at Usher and Knobloch's syndromes.
Occurrence Specifics
- Occurs in people of all races and economic levels
- A 35-year-old woman has about a one in 350 chance of conceiving a child with Down syndrome
- The chance increases gradually to 1 in 100 by age 40
- At age 45 the incidence becomes approximately 1 in 30. The age of the mother does not seem to be linked to the risk of translocation.
(National Down Syndrome Society, 2017)
It is one of those conditions that does not discriminate. It can affect all different levels of socioeconomic status and race. It is interesting that a 35-year-old woman has about a one in 350 chance of conceiving a child with Down Syndrome. It gradually increases to one in 100 by age 40. By age 45, it is one in 30. This is interesting because the age of the mother does not seem to be linked to the risk of translocation.
Types of Down Syndrome
- 95% of the time there is the presence of a ‘free’ extra 21st chromosome
- This is called ‘Trisomy 21’ Down syndrome is usually caused by an error in cell division called “nondisjunction.”
- Prior to or at conception, a pair of 21st chromosomes in either the sperm or the egg fails to separate
- The extra chromosome is replicated in every cell of the body.
- 3-4% is due to extrachromosomal unbalanced translocation of the 21st chromosome
- A partial or full copy of chromosome 21 attaches to another chromosome
- Usually chromosome 14
- 1-2% due to a mix of two cell lines, some with the usual 46 chromosomes and the other with trisomy of the 21st chromosome
- MOSAICISM (or mosaic Down syndrome, may be more mildly affected)
(American Academy of Pediatrics, 2011)
The error is specifically called nondisjunction. In 95% of the cases, there is a free extra chromosome at the 21st chromosome. At conception or before conception, this pair of chromosomes (at 21) in either the sperm or the egg fail to separate. There is no way of knowing where the error is. So it is nothing that either parent has done, it is just there is an error in the gene. This chromosome is in every single cell of your body.
Figure 1 shows a representation of nondisjunction.
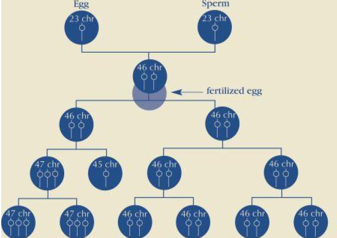
Figure 1. Representation of nondisjunction. Photo used with permission from NDSS.org
In 3 to 4%, this particular error is due to extrachromosomal unbalanced translocation of it. This is a more rare form. Remember with 95% of the cases there was an extra free chromosome. Now, in 3 to 4% of the cases, it is due to extrachromosomal translocation. That is when a partial or full copy is going to attach to another chromosome. It is usually on chromosome number 14. In 1 to 2% of the cases, it is due to a mix of two cell lines. In Mosaic Down syndrome, the individual is more mildly affected because it is a less severe error in the cell duplication. Hopefully that all makes sense to you, and if it does not, there are plenty of resources.
Statistics
- Once a woman has given birth to a baby with trisomy 21 (nondisjunction) or translocation, it is estimated that her chances of having another baby with trisomy 21 are 1 in 100 up until age 40.
- Remember that the likelihood of the first child with the condition is 1 in 700 infants
- The risk of recurrence of translocation is about 3% if the father is the carrier and 10-15% if the mother is the carrier.
- Genetic counseling can determine the origin of translocation.
(National Down Syndrome Society, 2017)
Once a woman has given birth to a baby with Down syndrome, it is estimated that her chances of having another baby with Down syndrome go to one in 100, up until 40. It definitely increases once there is a predisposition to having this error. For translocation, it is 10-15 % if the mother is the carrier versus 3% if the father is the carrier.
Genetic counseling is important to help support the family. It can help them to make the decision if they want to add to their family or not.
Diagnosis
- Prenatally
- CVS first trimester between 9 and 14 weeks gestation
- Amniocentesis during the second trimester between 15 and 20 weeks gestation
- At birth
- Identification of physical characteristics such as flattened facial profile, an upward slant to the eyes, single deep crease in palm of the hand, low muscle tone
- Completion of karyotype from a blood sample
- FISH test
Prenatally, they can diagnosis via chorionic villus sampling or CVS. This test is performed in the first trimester between nine and 14 weeks of gestation. With this test, Down syndrome can be detected early on because every one of those cells has the trisomy of the 21st chromosome. If a family chooses not to have a CVS or an amniocentesis, then they might wait until birth. This can be detected by way of physical characteristics. They also have to confirm it with a karyotype from a blood sample, and then sometimes they can use a genetic test called a FISH test.
At Birth
- Brain structure and function is NOT fixed at birth. It can be influenced by activity, social, early intervention, etc.
- We know children with Down syndrome will be delayed so use their individual baseline.
- Babies should have an eye and an ear test
- Compassion and reassurance for the family
- Discuss brain plasticity and the importance of early intervention with families
Many times after a diagnosis of Down syndrome, parents think this is it for their child. Remember, the brain has plasticity. We can change some of these pathways. We know that there is going to be a predisposition to certain things because of the genetic makeup of the condition; however, we can implement some changes that can help these children to function better as adults.
The brain structure is not fixed at birth. There are many things that influence a developing brain. Let's just say a baby is born in China. He or she can speak Chinese and learn all things about that culture, while another baby born and raised in the United States might learn both Polish and English and different customs. There is certainly a lot of plasticity and influence that we have as parents and through the environment.
We know that these kids are going to have a certain type of development as it is predictable with this condition, but we can help intervene at specific times.
Eye and ear tests are also so important for these kids. There are some specific genetic components that influence they eyes and ears that reside on that 21st chromosome. We cannot work on visual perceptual tasks if the child has functional and structural deficits that need to be addressed. As therapists, we work with a whole person. We need to have compassion and help advocate for these kids and families.
