Understanding the Who?
- Migrants = individuals who move from one place to another for any number of reasons
- Types of migrants:
- Asylum seekers
- Immigrants
- Refugees
To get started, I would like to start with a macro perspective of migrants. Migrants are individuals who move from one place to another. There can be several different types of migrants. Specifically, for this talk, we will be discussing refugees as a focus.
What's the Difference?
- Immigrants
- Individuals who migrate away from countries of origin
- Reasons may include:
- economic, political, health, or education.
- Asylum Seekers
- Seeking protection
- Application process
- Considered to be a voluntary act
- Can take years
- Can be denied
Understanding the different types of migrants gives us a perspective about the experiences that they all face when being resettled in different countries or voluntarily moving from one place to the next. This depends on their personal or group circumstances. Immigrants are individuals who migrate away from their countries of origin. Reasons may include economic, political, health, or educational reasons.
Asylum seekers want protection by being hosted in a different setting. They are looking for a new life and opportunities. These two types of migrants (immigrants and asylum seekers) are considered to be voluntary. This defines their experience when it comes to migration and resettlement.
Refugees
- Subset of migrants
- Forcibly Displaced
- Relocated
Refugees are a particular type of migrant. They are considered a subset and defined specifically by their forced displacement from one location to another. They are relocated by a third-party country or organization. Many times, they are forced out of their homes. This defines what their experiences are in terms of pre-resettlement and post-resettlement trauma.
- Internally displaced
- Within borders of the country of origin
- Externally displaced
- Cross international borders
Refugees can be further divided into two subgroups, either internally displaced or externally displaced refugees. Internally displaced refugees are relocated within their countries of origin. That means they might go from one territory to another, but they stay within their international borders. While externally displaced refugees cross international borders, they might be relocated by a third-party organization, a third-party military, or have to make the trek on their own, possibly into refugee camps. As we know, refugees are accepted in many countries across the world. They are generally relocated into countries that are close in proximity. However, the United States of America and other first-world countries with larger economic systems generally will house them in third-party locations with the opportunity to go back if possible. That said, it generally does not work out that way, and people are generally exiled from their original locations. They then build lives in separate and third-party locations.
Current Refugee Population Status
- 70.8 million displaced persons globally (UNHCR, 2019)
- 25.9 million are considered refugees (UNHCR, 2020)
- Refugee admissions in the U.S. have been in a steady decline (Carratella & Mathema, 2020).
- Numbers will dramatically increase in 2021 (UNHCR, 2020).
There are over 70 million displaced persons globally, and approximately 26 million of those are considered to be refugees.
2021 Refugee Admissions
- Report to the Committees on the Judiciary of the House of Representatives and of the Senate proposes:
- An increase in the number of refugees accepted into the United States in 2021 to 62,500
In recent years, the refugee population admissions declined within the United States. Now in 2021, as a new administration has come in, the numbers have dramatically increased from around 30,000 individuals to about 62,500. This increase is obviously due to political changes and policies. Prior to this, there was a little bit less funding allocated to accepting refugees into the United States. This is an example of how new political parties or regimes come into power and how perspectives and policies change. This all helps to shape some of the services for this population.
Prioritizing Refugee Admissions
- Will be prioritized by :
- Referrals for individual circumstances and need
- Group referrals for circumstance and need
- Individual cases from designated nationalities granted access for family reunification
When you have these different perspectives and ideas about how to prioritize letting people into the United States, there is a diversity of circumstances. Right now, admissions are prioritized based on referrals and individual and group needs. An example is a pandemic. Another is civil war. We may see migration and resettlement due to these circumstances.
2021 Refugee Resettlement
- Allocation of Refugee Resettlement FY 2021
- Persecution or fear of persecution
- Refugees falling under alien status based on the Iraq Act of 2007, Title XII, Div. A, Public Law
- Qualified residents from El Salvador, Guatemala, and/or Honduras
Refugee resettlement and allocation of resettlement is based specifically as of 2021 on persecution or fear of persecution, as well as specific alien statuses. These are based on the Iraq Act of 2007, Title XII, and Division A, as well as public law and international law that governs the relocation of individuals from country to country. Other qualified residents may come from El Salvador, Guatemala, and Honduras. This depends on both the perspectives and relationships between governments and whatever level of assistance the United States may be providing to friends or allies.
2021 Admissions: By the Numbers
- Based on the Following Regions
- Africa (22k)
- East Asia (6k)
- Europe and Central Asia (4k)
- Latin America/Caribbean (5k)
- Near East/South Asia (13k)
- Reserve Openings (12.5k)
- Total= 62,500 admissions
In terms of admissions from each country, there was a total of 62,500 coming from various areas in 2021. The new administration has made it a point to focus on several areas around the globe that need specific assistance for health, sequencing, and opportunities based on partnerships. A large number of this population has been coming from Arabic-speaking countries. You do not see it on here specifically as this is based on geographical location. Through my research and understanding, you can see that they generally come from middle Asian and African areas, with Northern Africa being the largest proponent.
Current Refugee Resettlement System
- Government agencies, partners, and funding
- Agencies
- Office of Refugee Resettlement, United States Citizenship and Immigration Services, Bureau of Population, Refugee, and Migration (PRM)
- Partners
- Refugee Council, Non-profit organizations, Religious organizations, etc.…
- Funding
- Federal/state grants, philanthropy, volunteers, and private donations
- Agencies
As we look at refugee resettlement as a whole, we want to look at the partnerships, the agreements, and the community as a whole in order to understand how these interacting factors take place and relate to one another. The current refugee resettlement system is built out of government agencies, partners, and private and government funding. Above I have listed a couple of agencies. Funding takes place through state and federal grants, private donations, philanthropy, and the work of volunteers.
Current System: Office of Refugee Resettlement (ORR)
- Partner Organization:
- Administration for Children and Families
- Core Services
- Health
- Employment/Economic Services
- Integration
- Unaccompanied Refugee Minors
To go into a little bit more detail regarding partner organizations, I would like to first take a look at the Office of Refugee Resettlement. This particular agency deals with coordination and communication between partner organizations. Their focus is mainly on core services such as initial health care, health status, employment economic services, integration, and unaccompanied refugee minors.
As we look at the Office of Refugee Resettlement, we can see that the core services, health, and integration as they relate to specific initial needs.
- Core services- Initial monetary needs
- Health- Initial health screening and insurance
- Integration- Initial economic/employment and education
We see that core services relate to initial monetary needs, whether it be housing or cash assistance. Next, we look at health screening and insurance, especially as it relates to people coming in from different geographical areas and experiencing different health status outcomes. We do not want people to bring in different types of diseases or viruses that are not native to the United States, putting the native population at risk.
Integration is really important because this is the main topic of what we will be discussing moving forward in this presentation. Initial economic/employment status, as well as education, are the main focus of integration services, whether it be from the Office of Refugee Resettlement or partner organizations and non-governmental organizations (NGOs) within your local state or national areas.
Current System: Government Partners
- Resettlement Agencies
- Church World Service/Immigration and Refugee Program, New York NY Visit disclaimer page
- Domestic and Foreign Missionary Society of the Protestant Episcopal Church of the U.S.A., New York, NY Visit disclaimer page
- Ethiopian Community Development Council, Inc./Refugee Resettlement Program, Arlington VA Visit disclaimer page
- HIAS, Inc. (Hebrew Immigrant Aid Society)/Refugee and Immigrant Services, New York NY Visit disclaimer page
- International Rescue Committee/Resettlement, New York NY Visit disclaimer page
- Lutheran Immigration and Refugee Service, Baltimore MD Visit disclaimer page
- U.S. Conference of Catholic Bishops, Washington DC Visit disclaimer page
- U.S. Committee for Refugees and Immigrants, Arlington VA Visit disclaimer page
- World Relief Corporation of National Association of Evangelicals/Refugee & Immigration Programs, Baltimore MD
This is a list of current government partners, as you heard in my introduction. I am currently working with Atlas Immigration Foundation. This is not a government partner, but they do have government contracts related to immigration administration, which is a large portion of what some of these government partners may do. It is giving people the opportunity to gain legal status, which is a large barrier for this population.
Current System: Funding Services
- Funding awarded to states and state-alternative programs
- In accordance with 45 CFR Part 400, Subpart I
- Based on the ORR equation
- Up to 60 months
- It varies from state to state
Current system funding is really important because, although you have state and federal funding in accordance with specific international and national law within the United States, a lot of the funding is based on the Office of Refugee Resettlement (ORR) equation. They do not necessarily make this equation public, but it is something that you might be able to research. This funding is only available for up to 60 months for refugees or those who have been resettled into the United States. This funding may vary from state to state depending on local or state regulations and depends on how many individuals that particular state takes in or needs to provide services to. The circumstances of resettlement are really important when it comes to state and federal funding.
Refugees and Forced Displacement
- What is forced displacement?
- An involuntary migration of people (Schuettler, K., & Verme, P., 2019)
- What causes forced displacement?
- violent conflict,
- economic and political instability,
- and climate change
(Algado et al., 2019; Boyle, 2014; Huot et al., 2016; Hynie, 2018).
Now, we can move into the distinction that makes refugees such a specific type of subset when it relates to resettlement. Refugees are particularly vulnerable because they face something called forced displacement. This is an involuntary migration of people, whether it be by violent conflict, economic and political instability, or climate change. We can see other things like a pandemic where you see people from South America or different countries who do not necessarily have the infrastructure to house people through situations.
- How does forced displacement affect the refugee population?
- Higher rate of physical and mental stress as (Hameed, S., Sadiq, A., & Din, A. U., 2019; Jamil et al., 2007).
- High levels of psychological, physical, and emotional distress as a result of forced displacement (Huot, Kelly, & Park, 2016).
- A distinct susceptibility to systemic barriers (Matlin, Depoux, Flahault, Saso, & Schütte 2018).
We also see that forced displacement can affect the refugee population in several ways, but none is more important than the higher rates of physical and mental distress. We see that psychological, physical, and emotional distress are distinct characteristics of this population as they are resettled into new countries. It makes them susceptible to systemic barriers that exist in whatever host country they end up being placed in. Specifically, in the United States, due to the complexity of social networks and understandings of economic systems, they face many systemic barriers.
Refugee Integration
- Political, social, economic, and cultural structures shape health services afforded to refugees (Ardon & Doormernik, 2018; Depoux et al., 2018; Durocher et al., 2016; Hammell, 2020; Hynie, 2018)
- Gaps in Care
- Integration/resettlement services lack the knowledge of human occupation and occupational rights (Durocher et al., 2016)
- Where is there a need?:
- Identification and analysis of current stakeholders (Knipper, 2018)
- Systemic frameworks, and (Knipper, 2018)
- Research findings to guide health policies and care (Knipper, 2018)
Refugee integration is shaped by political, social, and economic structures. There is a clear lack of knowledge regarding human occupation and occupational rights within the refugee integration system. Although they focus on some areas of occupation, it is perceived in a vacuum as opposed to being a holistic perspective of how an individual experiences their life and their existence.
- Where is the need?
- Identification and analysis of:
- current stakeholders
- systemic frameworks, and
- research findings to guide health policies and care
- Identification and analysis of:
(Knipper, 2018)
To dive in a little bit more deeply into some of the needs that relate to integration, we have to think about identifying and analyzing current stakeholders, system frameworks, and research findings to guide health policies. All of these areas are pieces of the puzzle and contribute to the function of an individual when they are resettled into a new setting. We need to also understand current stakeholders such as physical therapists who might work with people's physical needs. Mental health care may include occupational therapists, psychotherapists, or family therapists that are involved in helping with the adjustment period during which someone is forcibly removed from a place that they have known their entire life and is placed into a new setting.
There are also system frameworks to consider and how occupation is infused into the very nature of what these services provide. We know that these organizations provide English language training, whether it be as a second language or additional training for people to pass the citizen-level status. There is also an opportunity for people to receive health care (mental or physical), especially if they are coming from war zones.
There are policies based on research to make things a little bit more culturally competent and sensitive to populations that are coming into the United States. This is an additional piece of the puzzle that tends to get forgotten. As people get resettled, they have to then build their life within a new setting.
Challenges Facing Refugees
- Displacement and subsequent migration present transitional challenges to refugees resettled into host communities (Huot et al., 2016).
- Challenges are found at various stages of resettlement (Depoux et al., 2018).
- Challenges facing refugees affect
- resettlement in host countries,
- limiting occupational opportunities,
- and decrease overall health and well being
(Algado et al., 2019; Bloem & Loveridge, 2018; Depoux et al., 2018).
The challenges that refugees face because of displacement are based on the various stages of resettlement. There has to be an adaptation to multiple settings, whether it be in the host country or refugee camps. There are also limited occupational opportunities and a decrease in overall health and well-being because of some of these challenges and transitionary opportunities.
Stages of Resettlement
- Pre-Resettlement
- Sociopolitical contexts
- Climate/geography
- Educational and socioeconomic status
- During Resettlement Process
- Environmental circumstances
- Modes of travel
- Traumatic events
- Unsafe conditions
- Post Resettlement
- Adaptation to new circumstances
- Legal status
- Socio-cultural barriers
Taking a look at the various stages and some of the challenges that this population faces in these stages is really important (Figure 1).
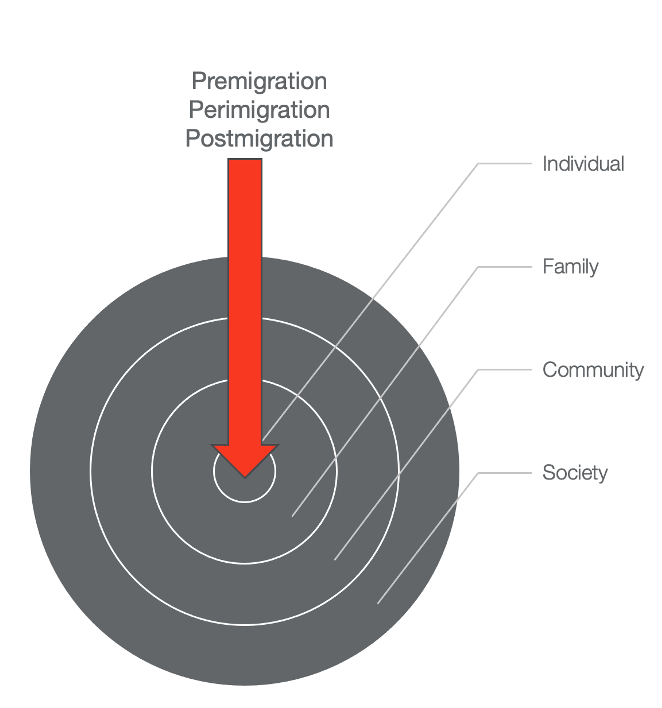
Figure 1. All stages of migration are affected at different levels, such as the individual, family, community, and society.
The pre-resettlement or premigration stage may involve many levels, including the social-political, climate and geography, and educational socio-economic status particular to their countries of origin. We understand that everybody comes with different cultural perspectives but being forced to relieve yourself of those cultural perspectives is a very difficult transition to make and not something that occupational therapy and therapists believe should be forced upon individuals when being resettled into new settings. During resettlement, there are many environmental circumstances such as modes of travel (by foot, by car, or by airplane) or traumatic events such as civil war or climate change (tsunamis, monsoons, or droughts, depending on the location). These can cause severe disruptions to the individual, family, community, and social networks. This also creates unsafe conditions, which cause people to think differently. It becomes more about survival as opposed to progression and development.
Challenges to Refugees: Post Resettlement Barriers
- Resettlement policies create barriers to performance and participation in host countries due to
- ambiguities in policy,
- limitations in service design,
- education, and
- training (Bloem & Loveridge, 2016; Depoux et al., 2018; Rubenstein, 2016).
Post resettlement is what we will be focusing on today as we are going to look at the United States system. We need to know how to help people to adapt to their new settings and obtain legal status through the socio-cultural barriers that exist. These challenges are emphasized or compounded by the policies in the United States. Many policies about international resettlement create barriers to performance and participation. There are lots of ambiguities between the national, state, and local levels, for instance. This creates limitations in service design and services provided to this population. It also limits the education and training levels of non-medical and medical personnel dealing with this population. There are also risks for marginalization, cultural imbalances, and socio-economic inequality. Due to the social complexities within the United States, this creates barriers and affects the prosperity of the population being resettled. It also shapes public opinion.
When we look at oppression and some of the injustices that people face, we see that many aspects intersect. They create a winding road of barriers for people to participate in a new setting. Gender, class, sexual orientation, ability, and nationality shape how people view the world and participate in their own existence. We also see that these can be reasons for people to leave their countries of origin because of the oppressions they feel. Thus, they come with a certain level of perspective, hoping that they can be treated and accepted in a particular way. Many times, communities are unsure or unaware of some of these complexities. This tends to create even more barriers to growth and prosperity.
Marginalization
- The World Federation of Occupational Therapy considers refugees to be a marginalized population (Algado et al., 2019)
- Marginalization leads to occurrences of occupational injustices (Huot, Kelly, & Park, 2016).
- The results of marginalization ultimately result in several forms of systemic disempowerment.
- Refugees lack agency, face social exclusion, and decreased health
- Limitations in performance/independence
Let's take a look at the marginalization of refugees. The World Federation of Occupational Therapy (WFOT) considers this population to be a marginalized population. We also have to understand that if we are looking at it from an occupational therapy lens, we can see that the occurrences of occupational injustice increase as it pertains to marginalization. The results of this type of marginalization, whether it be occupational injustices or social injustices, create systemic disempowerment. This limits the agency of refugees, increases social exclusion, and limits their opportunities for performance and independence within their new settings.
- Systemic disempowerment leads to:
- A lack of agency/autonomy,
- Social exclusion and
- Decreased health outcomes
Marginalization leads to the occurrence of systemic disempowerment, as we spoke about in the previous slide, but specifically, all of these areas lead to decreased health outcomes, whether it be mental, physical, or emotional.
Mental Health
- Higher rate of physical and mental stress as a result of:
- extreme suffering from the accumulative effects of physical and mental trauma, geological and cultural displacement (Hameed, S., Sadiq, A., & Din, A. U., 2019; Jamil et al., 2007).
- Stress incurred by new settings, cultural practices, and unfamiliar or non-existent support systems:
- Compounds traumatic experiences; leading to secondary psychological trauma
Mental health is a very important aspect to the resettlement process because refugees experience a higher rate of mental distress due to the accumulated traumas over time, whether it be from the initial resettlement process when they were displaced from their countries of origin or the new adaptation to settings and the stress incurred while trying to develop an understanding of new cultural practices and unfamiliar or non-existent support systems. As we see the initial trauma being based out of their countries of origin, we see that this population can also be subjected to secondary and tertiary types of trauma which compound or reinforce their original experience, whether it be displacement or migration.
- Premigration Trauma and Post-Resettlement Context lead to:
- Post-traumatic stress
- Depression
- Separation anxiety (Din et al., 2019; Kim, 2016)
- Additional Psychological Outcomes:
- Misalignment between role-identity and role expectations
- Dissatisfaction with occupational performance
- Temporal disruptions (Darawsheh, 2019)
The mental health status of this population, as we stated before, is based on pre-migration trauma in conjunction with post resettlement contexts. This population experiences high rates of PTSD, depression, and separation anxiety. Additional outcomes might be a misalignment with role identity and role expectations within new settings and decreased self-efficacy and with their occupational performance. I cannot emphasize this enough. Temporal disruption, or the timing of our society, is a shift from what people are generally used to within their countries of origin. In terms of temporal disruptions, we see that the timing sequencing and understanding of how social networks work within the United States cause a high level of dissatisfaction with the overall performance of this population.
Occupational Justice
- What is Occupational Justice?
- A conceptual tool for human rights advocacy (WFOT, 2018)
- The right of individuals to fully and equitable participation in diverse and meaningful occupations (Wilcock & Townsend, 2009).
- Occupational Justice promotes:
- Fairness
- Equity
- Empowerment
(Durocher et al., 2014)
Occupational justice adheres to and possesses principles of social justice. In occupational therapy, we can see them as the same thing or as equal because what we are trying to do is recognize the rights of individuals, whether they be at the lower economic status or higher economic status, with whatever skills they possess. People should be afforded the opportunities to participate fully and equitably within occupational or within occupations.
As we look at occupational justice and social justice, we see that they are both conceptual tools for human rights advocacy. We see that people have the right to fully and equitably participate in meaningful occupations. Occupational justice, in particular, focuses mainly on the fairness, equity, and empowerment of individuals to participate not only in occupations that they have previously found meaningful but the ability to transition those previously held meanings into new settings. This is being able to appropriate those particular meaningful occupations into an environment that is conducive and open to them participating fully within it.
Occupational Injustice
- The restriction of occupational rights to meaningfully participate and contribute to individual and community wellbeing reflects occupational injustice (Hammell, 2020).
Occupational injustice can be seen as several types of road bumps. There are potholes, speed bumps, stop and yield signs, and so on. The restriction on people's occupational rights is similar as some are big and some are small. You also need to have the skills to avoid or move through them. We need to provide skills to the refugee population in order for them to successfully navigate injustices and systemic barriers that they face when being resettled into a new country or setting.
Types of Occupational Injustice
- Occupational Apartheid
- Occupational Deprivation
- Occupational Alienation
- Occupational Imbalance
- Occupational Marginalization
And so, as we look at occupational injustice, we see the different types of injustices that occur. We see occupational deprivation, alienation, imbalance, marginalization, and apartheid.
Occupational Marginalization
- Definition:
- Individuals are excluded from occupational participation based on social norms and expectations (Durocher et al., 2016).
- Occupational Right:
- The right to possess autonomous participation in occupations
- The right to external occupational autonomy
- How does this affect refugees?:
- Lack of access
- Lack of agency
- Lack of decision making
We are going to first start with occupational marginalization since we have discussed it previously. We focused a little bit on the perspective of marginalization as it relates to this population being placed into new systems. We see that the occupational right that is challenged is the possession of autonomy as it relates to participation in occupations as well as the right to externally determine what their autonomy level is. What we see is this affects refugees in terms of access to certain support systems and services and agency over their own existence. We want this population to be agents of their own change as well as have decision-making capability as it relates to their participation, whether it be in work, leisure, or social participation.
Occupational Deprivation
- Definition:
- Individuals are restricted from occupations outside of their personal and immediate control (Durocher et al., 2016).
- Occupational Right:
- The right to increased health and well-being through participation in occupations
- The right to develop through participation in occupations for health and social inclusion
- How does this affect refugees?:
- Limited participation
- Decreased or absence of meaning
Occupational deprivation is where individuals are restricted from occupations outside of their immediate control, and this is where deprivation occurs. What ends up happening is we see limited participation within social work or leisure networks as well as a decrease or absence of meaning for individuals when it comes to their participation in occupational activities.
Occupational Imbalance
- Definition:
- When too much time is spent in one area of occupation over another; or occupational opportunities are afforded more heavily toward some individuals than others (Durocher et al., 2016)
- Occupational Right:
- The right to benefit from privileges or advantages associated with occupational participation and performance
- The right to prosper from diverse occupational participation
- How does this affect refugees?:
- Lack of alignment
Occupational imbalance, as we discussed before, can be a misalignment between role identity and role expectations. As people transition themselves into new settings, we see that their previously held roles, rituals, and routines, which had generally become habits over time, become disrupted. With that disruption becomes a decreased level of self-efficacy and self-identity, in terms of their familiar roles within their family and community.
Occupational Alienation
- Definition:
- Individuals face experiences that lack meaning and ultimately create isolation, disconnect, or emptiness as a result of limited opportunities for self-expression (Durocher et al., 2016).
- Occupational Right:
- The right to occupational experiences that are meaningful and enriching to the individual
- The right to enriching occupational experiences
- How does this affect refugees?:
- Isolation
- Exclusion
- Lack of fulfillment
Occupational alienation, in my view, is related to the settings that people are placed in. They experience a lack of meaning and enrichment of their individual selves, as well as face experiences of isolation, exclusion, and lack of fulfillment. This could be from social structures within local settings, a general national view of who they are as individuals based upon their refugee status, as well as maybe being placed in settings without their family or friends. It changes how they view themselves in relation to the world around them.
Occupational Apartheid
- Definition:
- Occupational participation is restricted based on race, ethnicity, nationality, social status, age, gender, etc.… (Durocher et al., 2016).
- Occupational Right:
- The right to meaningful and purposeful activity regardless of social, political, or economic status
- The right to meaningful and purpose full occupational participation
- How does this affect refugees?:
- Social, political, and economic exclusion
Occupational apartheid is something that exists in the world. I think we all commonly understand it from the South African apartheid. It relates to the meaning of purposeful activity regardless of social, political, or economic status. When somebody experiences occupational apartheid, their participation is restricted based on anything that makes them who they are whether it is race, ethnicity, nationality, social status, age, or gender. I know that this is not a very common form of occupational injustice, but it does exist. It is something to keep in mind when you are dealing with this population in terms of being resettled into the United States, since we do take on such a diverse group of individuals every fiscal year.
Why Is This Important to Occupational Therapy?
- Therapeutic use of life activities when caring for individuals, groups, populations, or organizations to support participation, performance, and function within activities and contexts that are meaningful (OTPF, 2020).
- Services can be impactful within both medical/clinical settings
- Social practices
- The possession of community support and social inclusion
- Social participation, mental health, self-determination, life skills, and performance patterns
(Algado et al., 2019; Aranhan et al., 2019; Arslan et al. 2018; Darawsheh, 2019; de Mello et al., 2020; Galvaan & Richards, 2018; Huot et al., 2016)
We all know the definition of what occupational therapy is in terms of caring for individuals, groups, and populations. It is also infusing ourselves into organizational structures, becoming translators of culture and society, as well as providing community support and inclusion through social participation, mental health, self-determination, life skills, and performance patterns. It is vitally important to the coming generation of individuals who find themselves resettled into the United States.
Challenges to Refugees Addressed by Occupational Therapy
- Instrumental Activities of Daily Living
- economics,
- healthcare,
- community supports,
- dietary challenges,
- education
- employment
(Arslon et al., 2018; Depoux et al., 2018; Huot et al., 2016)
- Performance Patterns
- familiar occupational roles,
- rituals,
- routines,
- habits
(Darawsheh, 2019; Huot et al., 2016; Mahoney & Siyambalapitiya, 2017) Taking a look at the OTPF, we can see the specific areas of occupation which are most highlighted in my past research as well as my capstone project. We can look at instrumental activities of daily living or the activities that support life. We can also look at education, employment, and healthcare. What you do not see is training in terms of healthcare comprehension. You do not see training in terms of building community support. You might see an understanding of the challenges that face people when transitioning into new cultures, but you do not necessarily see the specificity when it comes to the actual services they are being provided. They are being given every opportunity, like supplies that are provided to them, but they may not have the same cultural perspective that exists when it comes to that. Also, taking a look at performance patterns, they do tend to shift in terms of familiar occupational roles, rituals, routines, and habits, as well as how we translate those roles into new settings because of the temporal disruptions that we discussed earlier in this presentation.
Client Factors
- Values, Beliefs, and Spirituality
- Body Functions
- Mental Functions
- Performance Skills
- Processing
- Social Interaction
- Contexts and Environments
- Personal, Temporal, Virtual, Social, Physical, Cultural
Client factors, performance skills, and contexts and environments are really important to assess in this particular population. Obviously, people come with different values, beliefs, and spirituality. As occupational therapists, we may need to shift our roles about how we translate culture in regards to people's particular mental status, and their ability to participate in some of the routines that exist within the values, beliefs, and spirituality they already hold. This can perhaps open up new doors for them to participate in new contexts and environments.
Theoretical Frame of Thought
- Applied System Theory
- Interpretation of interactions within complex systems
- A whole system possessing various subsystems
- Utilized within the health care system
- MOHO
- Models of Practice
- MOHO
- PEOP
The theoretical frame of thought that I have applied to this particular presentation, as well as the models of practice, is the Applied System Theory. Applied System Theory deals with the interpretation of interactions within complex systems. Applied System Theory has contributing subsystems. In my estimation, the whole system can be considered the refugee resettlement complex, and subsystems such as occupational therapy, physical therapy, psychotherapy, caseworkers, or anybody who participates within the system, can be considered a subsystem that contributes to the overall function of refugee resettlement. As we look at utilizing health care systems within this framework, we see that occupational therapy, because of its broad-based perspective and outlook on therapy, integration, and participation, can be a vital role in terms of creating collaboration between these different types of services as well as the models of practice.
Particular models of practice that I find most helpful within the Applied System Theory are MOHO and PEOP. I chose MOHO because a common misconception when it relates to this population has to do with volitional choice. As we have seen throughout the presentation, volitional choice is very important to finding meaning and perspective in terms of occupational choice. Being able to determine where you go, when you do it, and how you do it is vital to meaningful perspectives and experiences. And, in conjunction with that, PEOP looks at the environmental aspect. This is the person interacting with their new environment, and I think it provides a needed perspective as it relates to the needs of the population as they transition into new settings or new environments.
Future Vision
- Where does occupational therapy fit into refugee integration services?
- Advocacy
- Research
- Organizational Coordination
- Policy
The future vision for occupational therapy, I believe, falls along the lines of advocacy and research into more culturally sensitive perspectives for this population. There also needs to be organizational coordination between all partners within the United States. Although people provide specific types of services, the main focus is related to education and employment. As occupational therapists, we can advocate for these populations and help to shift general political perspectives as they relate to access to services, the opportunity for participation, and the means for growth within new settings.
In terms of future implications, I think that as a profession, we can look at minority health as something to address, whether it be through policy change or whether it be via group or health community supports. We can look at health disparities that exist within the framework of our society, whether it be based upon minority health or marginalization, and look at the injustices that create these health disparities. I think that educating medical and non-medical personnel, whether it be from a cultural competency standpoint or from an occupational therapy perspective can help to transition people through trauma into trauma recovery. I think another aspect we can tap into is the recovery model. This is becoming more popular within mental health services. It looks specifically at self-agency, self-reliance, and independence. Thus, I think it fits in really nicely in terms of the integration challenges that these individuals face either from mental health or an integration standpoint. It incorporates the areas of transition that are most important to individuals, groups, and populations, as they are forced out of commonly adhered to values, beliefs, and cultural roles. I think that looking at this population from a recovery perspective, as opposed to them having a condition that needs to be treated, might give us the best long-term perspective.
I would like to go back to the occupational deprivation of this population. In my experience, limited participation and the absence of meaning for this population create a disruption to how they view systems. When they are placed into a new social system, their limited access or participation, whether it be through work or education, also limits their skillset within the new setting. I think that we can all agree that as people go from one particular system to another, their understandings and opportunities need to be in their immediate control. And, if people lack immediate control over their perspectives and their participation, it will really hamper their ability to successfully prosper and participate within new societies.
For marginalization and the implication for occupational therapists, we see a shift back from a biomedical model into social perspectives or social justice so that we can provide more access. We can provide more agency and decision-making as it relates to resilience through trauma self-agency over experiences of disruption, limitations, restrictions, and the ability to really navigate some of these social barriers.
What I have found in my experiences working with this population and developing areas for growth is that they do not necessarily lack the skills, but rather they lack the opportunity. If we are able to advocate for this opportunity, it will give us more insight into long-term needs as opposed to these momentary lapses in occupational performance and participation.
Future Implications
- How does our work with this population expand our place inform future practice?
- Minority health
- Health disparities
- Cultural competency
- Education
In terms of the future implications for occupational therapy as a whole, I would like us to leave with a certain perspective in regard to how we should view not just refugees but other minority populations. As occupational therapists, we want to tread a path for other health care workers. We want to stake our claim to opportunities that exist for our profession. We should develop our role within the organizational structures as it will help us shape what services are provided, how they are provided, and how they are implemented in terms of the service structure within refugee resettlement opportunities. As occupational therapists, we are experts in human experience. We understand how people communicate, why people communicate, and in what forms and fashions people communicate. We possess a distinct skillset and understanding of populations. It does not have to be a population that is restricted, but because we are dealing with a social justice framework as it relates to refugees and looking at occupational justice in regard to that population, this will assist us in that growth. I think that utilizing our professional perspectives of assistance, advocacy, and support for this population will relate and translate better if we are able to obtain leadership positions so that we can not only shape the healthcare system but shape the system overall. I think that provides us a great opportunity for growth not only as individual therapists but as a community so that we can assist others in their growth and prosperity as it relates to participation and performance in occupations across the board.
Questions and Answers
How did you get interested in this topic?
I am a first-generation American. I am the son of immigrants and the grandchild of refugees. It gives me a unique perspective and understanding of what the experiences and challenges are as they relate to trying to prosper within new settings when transitioning.
When you were working on your capstone, I am sure you came across many different people that you worked with. Are there any specific cases during your research that you can highlight?
My research was based on the service structure as a whole. Occupational therapy services are non-existent within refugee resettlements. Although areas of occupation are utilized in terms of services provided, they are utilized in isolation with one another. Educational services and healthcare services are separated from one another as though they are independent of the human experience as opposed to being pieces of a whole. What I found was that the service providers, whether they be people who have created programs for this population or the people who are doing administrative work, do not possess a clear understanding of the importance of occupational meaning as it relates to overall success.
Were other professions involved?
There are social workers and caseworkers involved in cases. For example, there are high rates of domestic violence as it relates to immigrants, asylum seekers, and refugees. They are coming from different cultural perspectives and experiences. Thus, some of the commonly held beliefs or assumptions within one country shift in a new country. People lack the knowledge of their own personal rights and not necessarily knowing that they possess the right to live independently. They do not have to adhere to whatever previous perspectives they had.
Do you see OTs having a big role in working with children that are crossing the border from Mexico?
Yes, I do. When you asked me before about what other professionals I have interacted with, I had a participant in my research study that was a physician at one of the centers at the border where they are housing children. She had a lack of knowledge regarding occupational therapy in general. What I found recently in working with the Atlas Immigration Foundation and the partnerships they have created is that there is a need for occupational therapists to not just educate children but educate families as a whole.
How often do refugee families play a role in a refugee's integration?
I think you are asking what role the entirety of the family plays in integration. Refugee families, depending upon whether or not they were resettled together or separately, can play a large role in terms of mental health, physical health, and emotional health. Refugees are resettled as individuals as opposed to family units so that there can be a resettlement process that eases them into the new setting, but it does not necessarily take into account the complexities of cultural standing as it relates to the family unit and the importance they play in regard to somebody's ability to successfully navigate barriers with a particular support system.
What would you recommend for new grads or even experienced occupational therapists who want to work with refugees?
For new grads with student loans and who are establishing an independent living situation, the idea of not making money is daunting. In regard to working in this population, there are loan forgiveness programs related to working for 10 years or more within civil or nonprofit settings. This might be an incentive to work in this area.
It seems like this population might land itself to running some groups. Have you ever run any groups with this population?
I have not run a group yet, but I am in the process of building a mental health therapy program for not only domestic violence victims, but also want to extend it into the refugee population. I work at the Atlas Immigration Foundation in Pembroke Pines, working out of a community center that is owned by a local mosque. They build the community through their religious activities and social networks. They also are starting to tap into political, leisure, and work networks so that they can assist the population as they transition. I think this might be the best avenue as it views refugees from a perspective that they understand as opposed to just throwing information at them when it comes to the United States system.
Where would you begin to look to get an OT job with refugees?
My research is focused on building occupational therapy's role. I have not found any occupational therapy jobs with the refugee population outside of the organization that I am working with now. People have not employed occupational therapists within that setting. I believe it is because OT has not been an area explored in as much detail for leadership positions, group networking, or running a program itself.
What about refugees who have been here for a while and are trying to integrate into the communities? Do you see OTs working in those more established communities?
There was a study done regarding the dependence or the economic strain that refugee populations place on the host country. They were primarily looking at the United States. They found that because refugees lack extended support services, they also lack integration services in terms of how to integrate socially, economically, and politically. They also find themselves two to three times more dependent upon social programs than the native population. I think that is a great avenue for occupational therapists to find themselves in whether it be through the development of new skills or the reinforcement of old skills prior to resettlement.
How often did you find that occupational therapy refugee patients dealt with discrimination by other providers? What is the best way or method to advocate the patient without possibly causing insult to culture or to the patient?
I have not found that. Instead, what I have found is that refugees do not necessarily lack the understanding but rather experience with health care systems. There is a distinction between the global north and the global south. The global north is considered to be more westernized colonial powers including the United States, Great Britain, and Australia. They have specific types of health care systems that do not necessarily translate to whatever health care they were receiving in their countries of origin. This creates a lack of familiarity with this new system. They feel unsure about how to go through the processes of not just finding health care, which they have access to for the first eight to nine months of being resettled, but also being able to reapply and securing funding for healthcare.
Do have any advice on helping child refugees integrate into the public school systems?
There is a great paper by Bloem. They did a study regarding the challenges that face this population, and the education of child refugees is one of them. They found that an undue level of stress is placed on child refugees because they are trying to not only translate culture for themselves, but they are also trying to translate the barriers and challenges for their families. I think providing them the skills to communicate effectively and navigate social circumstances in regard to leisure and play is important. We need to give them opportunities to appreciate their own uniqueness but also how to integrate that uniqueness into a new environment.
I think children of refugees often become the main communicator for the family. Do you agree?
Yes. They are able to assimilate to the language quicker and they end up having to take on a parental role. To build on this, it is important to focus on training the educators and other adults that a child cannot always grasp the complexity of certain topics. You can give them some of those opportunities, but we also need to provide the parents the necessary services to fill those needed occupational roles.
How can a person become involved in your organization/foundation?
If anybody is interested in becoming a part of what I am doing with Atlas Immigration Foundation, feel free to email me. I can always put you into contact with the CEO of Atlas immigration Foundation, and we can communicate about the next steps in terms of how the operation is planning on being run and how we would like to fit occupational therapists within the framework of a leadership position.
References
Available in the handout.
Citation
Mrabe, K. (2021). Exploring the role of occupational therapy and refugees. OccupationalTherapy.com, Article 5457. Retrieved from http://OccupationalTherapy.com
