Amber: I am going to be speaking on the management of less common neurological disorders today. Many of us work with people with neurological issues, but maybe not some of the rare disorders that I am going to cover today. They are often called orphan disorders, simply because people feel like they are the red-headed stepchild. They do not get as much funding, attention, or research. I am going to go over a number of different disorders so that you can use this as a reference back, instead of just a few in-depth. You may not have a client with this disorder for five years, but after this course, you should have some information to guide your treatment. Most of the ones I am going to present today are progressive disorders, some slower than others. Many therapists treat people who are getting better. This is a whole different beast, to work with somebody who is not going to get better in the classic sense. Many times the OT practitioner may come across less common neurological conditions in their clients, and be unsure as to precautions and management. This course will provide an overview of uncommon progressive and static neurological conditions and OT practitioner management.
Rare Diseases Covered
This is the laundry list of some of the rare diseases I am going to cover.
- Multiple (Multi) System Atrophy (MSA)
- Progressive Supranuclear Palsy (PSP)
- Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)
- Multifocal Motor Neuropathy (MMN)
- Spastic Paraparesis
- Dermatomyositis/Polymyositis
- Inclusion Body Myositis (IBM)
- Post-Polio Syndrome
Certainly some are more rare than others. Some of them you may never have heard of and some of them you may treat folks with all the time, but in our clinic, we often see unusual disorders as we are next to a level one trauma center. Post-polio is the most common on this list, but certainly rare diseases in total impact a large number of people (30 million and 1/10 people), and some of these may come across your desk. For each diagnosis, I am going to have a basic overview slide, and then we will get into some of the occupational therapy specific issues. Thoughout, you will hear some common themes because there are similarities between the conditions. I will go through them and then answer any questions. If anybody has something to add to the discussion, please let me know.
Multiple (Multi) System Atrophy (MSA)
I am going to start with Multi System Atrophy, sometimes known as Multiple System Atrophy or MSA.
Overview
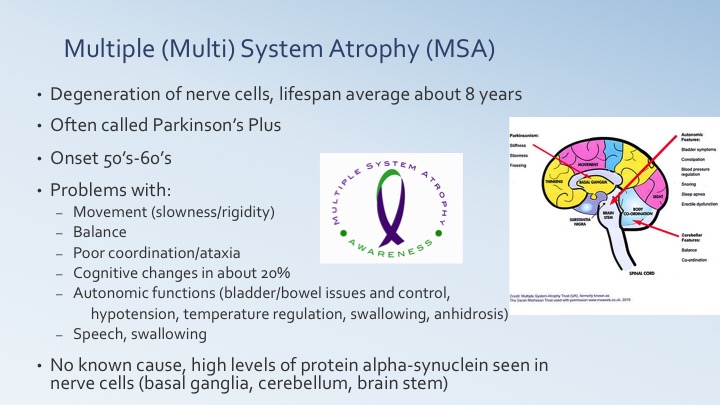
Figure 1. Overview of MSA.
It is linked in some ways with Parkinson's, and has been called a Parkinson's Plus disorder. It progresses faster and the life span on average is only eight years. Generally, Parkinson's does not have a life expectancy limit, unless somebody gets pneumonia or something. It is degeneration of nerve cells. It is sometimes confused with Parkinson's because there are movement problems with slowness, rigidity, and balance problems. Therse are some of the things that you would see with Parkinson's so a lot of times it gets misdiagnosed. There is a slightly earlier onset in the 50s and 60s, whereas Parkinson's is a little bit later. There are a couple of other diagnoses that are confused with Parkinson's as well that we will also discuss. There is a little more ataxia than you might see with Parkinson's. Clients have difficulty getting their muscles to behave in a coordinated fashion. It is not typically a tremor, but rather when they reach for something, their arm goes where they do not want it to go. There can also be some cognitive changes, but only about 20% in this group. They also often have significant autonomic problems. Even if you are moving around fairly well, if you have bowel control issues, that is a very big deal and can cause functional problems. The only one that you might not recognize right off the bat is anhidrosis, or difficulty with sweating. If you do not sweat, sometimes you can have significant temperature regulation problems. There can be some concerns with doing some leisure tasks because they might get overheated. There are almost always speech and swallowing deficits. They are not sure what the cause is, just as they do not really know what causes these deficis in Parkinson's. Nobody really knows with these rare and orphan diseases. I suspect because a lot of the times there is not money being spent on research, but they are seeing a higher level of a protein called alpha-synuclein in the basal ganglia, cerebellum, and brain stem. Potentially some of the treatments might be working toward dealing with those higher levels of protein.
MSA- OT Issues
Figure 2. OT intervention for MSA.
As you can see with this group, and honestly almost every group that we are talking about today, there is a fall risk. It is either a balance issues or a weakness issue. With this group, there also is the autonomic problem with the hypotension. They get up and they are immediately dizzy, and if they are not prepared, they are on the ground. Certainly, the lack of sweating and temperature problems can lead to heatstroke or overheating. Sometimes dehydration, along with swelling problems, can lead to some dehydration. If someone has urinary urgency, they are much less aware of safety issues. Cognition also plays a role in it. And then, if they cannot communicate appropriately, how do they get their needs met? How do they get help when they need those sorts of things.
Treatment I would suspect would most likely be at home, unless someone has a fall and breaks a hip. This could be a secondary diagnosis. This is often the way that the therapist will see folks with these sorts of disorders. With almost everybody, our focus is on ADL's and IADL's. With the slowness of motion and ataxia, they are going to have problems with fine motor tasks, like writing, buttoning, shoe tying, and managing pills. With ataxia, maybe their spoon is hitting the side of their face instead of their mouth. Think about how to manage some of those ADL tasks. If somebody gets MSA and they were relatively normal before and now within eight years, they are deceased, this is a fast pace of change. We need to help them problem solve how to continue to complete tasks as long as they can. As far as balance issues, you may need to put up a rail in the shower. They need strategies to manage the bradykinesia (slowness of motion) and the rigidity. They can also have that lack of initiation, similar to Parkinson's. Many people think slowness of movement equals slowness of thought, and that of course is not necessarily the case, although there can be some cognitive challenges. With decreased balance and coordination, there are going to be showering and toileting issues. They may need to sit to put on their clothes.
I see every plan of care that comes through our building, for all of our 14 neurologists, because I am the only OT here. A lot of times, therapists say there are no goals, or I hear therapists say that they are not going to see this person for more than a session or two. Today, I want to focus on the goals of treatment, as much as anything else, so that therapists feel like there is something to do. We can focus on home safety, whether it is because of the hypotension, balance problems, ataxia, or the bradykinesia (rigidity). Any of these issues can cause decreased safety awareness, as well as cognitive changes. Their occupations may include meal planning or opening containers from their Meals on Wheels. Perhaps they have to take care of a spouse, or they just have to be able to get out of bed safely. Many people with progressive disorders are going to need adaptive equipment (AE) and adaptive techniques. However, if somebody is very quickly progressing, it is also a challenge to recommend adaptive equipment because it may only work for a certain period of time. For example, maybe they can use a button hook for a short time, and then the button hook, because of ataxia, becomes too hard to coordinate. You may need to suggest something that might last a little longer and save some money. Velcro could be added behind the buttons, or they could do a snap shirt. Another option might just be a pullover shirt. We need to look ahead to come up with solutions. We also work a lot with the transfers and bed mobility, whether that is a different technique or working on safety.
Progressive Supranuclear Palsy (PSP)
Overview
The next one is Progressive Supranuclear Palsy, or PSP. I had a dear friend who had PSP, and it is a very interesting condition (Figure 3).
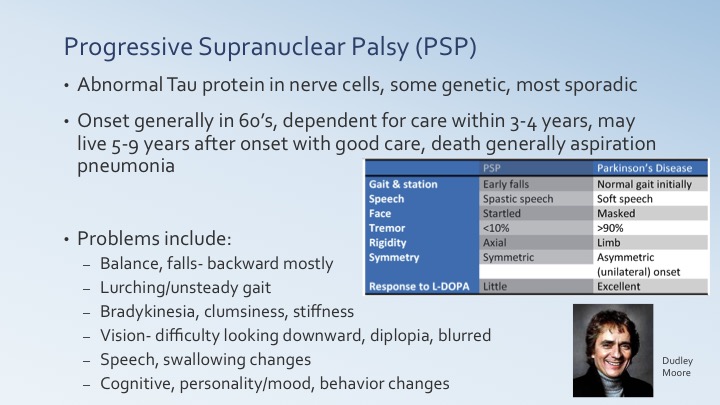
Figure 3. Overview of PSP.
PSP is often confused for Parkinson's disease, but it is not called a Parkinson's Plus. It is a unique disease, but there are some similarities. There are some difficulties or abnormalities with the Tau protein in some of the nerve cells. PSP can occasionally be genetic, but almost always is sporadic, and the cause is not known. My friend lived about five years after onset, thus it is a very quickly progressing disorder. The table in Figure 3 compares PSP and Parkinson's, and I probably should have done it with MSA as well, but this was one that was a more easily available. This can guide physicians and other health professionals. A person with PSP typically does not have the tremors. It is very symmetric, as compared to Parkinson's, and there is a different speech pattern. They often fall very early and almost always backwards, unlike those with Parkinson's who have normal gait initially. The gait seen with PSP is a weird lurchy, all over the place unsteadiness. In constrast, the gait seen in Parkinson's gets very tiny, with a festinating sort of motion. They can have the bradykinesia with the real slowness, but it is seen more as clumsiness. They might miss their face with a spoon, drop items from their hands, or are not hitting targets correctly. One of the hallmarks is significant vision issues. My friend could not look downward so she could not see obstacles in her path and that was a very very big issue. Luckily, she lived alone and could control this as far as toys and things around. However, depending on onset and family situation, this can be an issue. There are almost always speech and swallowing changes. My friend had a number of cognitive and personality changes. She was a very nice person, and she became very irritable and paranoid. She had a son who she thought was not helping her. Dudley Moore had PSP. Aspiration pneumonia, due to swallowing changes, is the main reason for death, but certainly there could be a fall or something like that as well.
PSP- OT Issues
Figure 4. OT intervention for PSP.
There are many precautions. Visual issues present many problems. We can use some visual strategies, like prism glasses, to be able to modify their vision slightly. There are also a lot of cognitive problems with this group. This ties in with safety for things like medical management and emergency access. Finally, there are swallowing precautions.
Some of the treatments are going to be maintaining range of motion and pain as a secondary process from being stiff. They many need some visual compensation for example if they have the double vision. You may want to use an opaque patch to be able to manage the double vision or prism glasses for decreased vision in the lower quadrant. The use of safety strategies becomes important such as: moving obstacles, securing rugs and cords, and those sorts of things. If they are going to have to do stairs, they may need a safety strategy for that. We will need to also assess balance for ADL and IADL tasks.
There are many OT goals. We may work on self-feeding and instruct in safe swallowing processes. Again, we need to look at home safety and ADL performance. Sometimes with this group it is more about strategies than a lot of adaptive equipment. How do we get on and off the toilet safely? How do we prevent falls? We may need to provide some patient and family education on the cognitive changes. Certainly a lot of these goals could pass back and forth between a number of these disorders. Finally, we need to look at visual strategies as part of our goals. If they are not able to look downward, how are they going to eat their food, manage their medications. etc. We need to do serial therapy; in small chunks off and on over time. You might see somebody for six weeks, on this particular set of goals, and then you go away. Then maybe six months or a year later, you need to go back because they have had a change in condition or a progression of the disease.
Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)
Overview
It is thought to be a chronic version of Guillain-Barre, which is sort of interesting. There is a graph in Figure 5 (little small), but you can get the idea between Guillain-Barre in the green and CIDP in the pink.
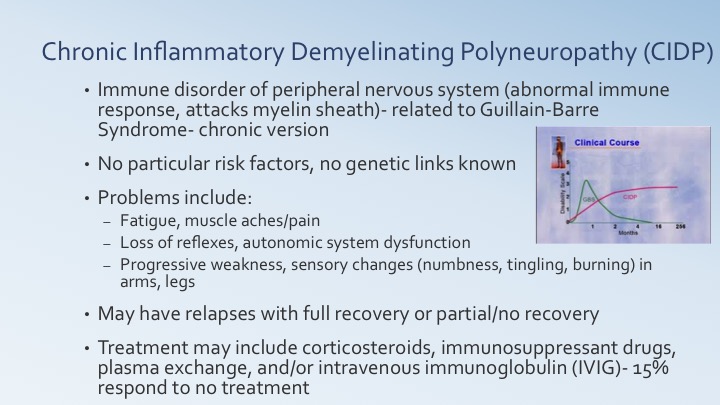
Figure 5. Overview of CIDP.
They think it is a similar process of an abnormal immune response. The disease attacks the myelin sheath in a similar way to Guillain-Barre. There are no particular risk factors or genetic links. It is not associated with a particular trauma, pneumonia or flu-shot that they have linked to Guillain-Barre. They cannot find as many of those risk factors. The problem tends to be with the peripheral nervous system where there is a loss of reflexes, weakness and sensory changes like numbness, tingling and burning. Typically, this is found in the hands and feet, and then it progresses up the arms and legs. Along with the weakness, they can have fatigue and muscle aches and pains. If somebody is used to performing at a certain level, the new weakness and fatigue can limit what people want to do. There can be a course with CIDP that relapses with full recovery, similar to MS. However, many times people do not fully recover. Instead, they might have a partial recovery or no recovery. It does tend to be a straight line like you see on the graph versus a lot of the up and down. With the abnormal immune responses, treatment includes corticosteroids, immunosuppressant drugs, plasma exchanges and intravenous immunoglogulin (IVIG). People need to keep up with that. Unfortunately, 15% of clients do not respond to treatment. It is slowly progressive, especially if those relapses do not lead to a full recovery each time.
CIDP-OT Issues
Figure 6. OT intervention for CIDP.
This one is a little tricky as far as treatment is concerned. If the person typically recovers, then you would want to do strengthening; however, you do not want to push too hard or cause them to overheat as that can cause a relapse. If they tend to be in a cycle with only partial recovery or no recovery, it may be more of an adaptation approach. Again, overheating, pushing and stress can cause a relapse. With sensation loss and weakness, safety can be an issue. They have to be careful of hot water or slips and falls. We need to help them gradually gain strength and endurance within those limits of not pushing too hard.
