Editor's note: This text-based course is a transcript of the webinar, Seating Considerations in the Home Health Setting, presented by Sara Frye, MS, OTR/L, ATP.
Learning Outcomes
After this course, participants will be able to identify at least two basic seating and positioning principles in order to identify postural supports for three common asymmetries.
After this course, participants will be able to identify three areas that should be assessed in a seating evaluation based on client, occupation, and environmental factors.
After this course, participants will be able to examine three logistical challenges and ethical considerations for seating and positioning in the home.
Introduction
My name is Sara Kate Frye and I am an OT with over 15 years of experience. I am happy to have the opportunity to talk about seating considerations in the home health setting. I am an occupational therapist with a broad inpatient rehabilitation background who transitioned to home health two years ago. One of the things that I noticed moving into the home health setting is the vast need for seating and positioning interventions. However, clinicians (and clients) often do not feel they have the tools to address these complex cases. My goal is to give you some ideas for interventions to be a more effective clinician and a better advocate for your patients, knowing that there are so many different things that we are triaging and addressing in the home health setting.
Background
Although there is a wealth of knowledge on seating and positioning, there is little evidence on seating and positioning in the home health setting.
Specialized seating clinics exist but may be inaccessible to clients who are homebound.
Conversely, clinicians working in home health may have limited knowledge and comfort in providing seating and positioning interventions.
There is a wealth of knowledge on seating and positioning; however, there is little evidence for seating and positioning in the home health setting. We are going to address this today. As I mentioned before, I have experience in inpatient rehabilitation and previously ran a seating clinic in a large inpatient rehabilitation hospital. As I transitioned to the home health setting, I needed to adapt those skills to the home health setting.
Specialized seating clinics exist, but often these clinics are inaccessible to our homebound clients. Even though home health clinicians may not have the most advanced training or knowledge, they are the clinicians in the home with the clients. As such, clinicians working in home health may feel that they have limited knowledge of providing seating and positioning interventions. Since they are the ones who are present in the home, they have to have a plan to address seating and positioning needs.
Today, I hope to give you a plan of attack for how you might triage some of these more complex seating and positioning cases.
Homebound Status
Criteria One (One of these must be met)
Because of illness or injury, need the aid of supportive devices such as crutches, cane, wheelchairs, and walkers; the use of special transportation; or the assistance of another person to leave their residence
Have a condition such that leaving his or her home is medically contraindicated
Criteria Two (Both must be met)
There must exist a normal inability to leave the home.
Leaving the home must require a considerable and taxing effort.
(Loeffler & Simpson, 2015)
For a definition of homebound status, I will use Medicare's criteria. Criteria one is that the client is homebound due to illness or injury and needs the aid of supportive devices, such as crutches, cane, wheelchair, walker, or the use of special transportation, or the assistance of another person to leave their residence. They may also have a condition where leaving their home is medically contraindicated.
Second, there must be a normal inability to leave home, and leaving home must require a considerable and taxing effort for the client.
Seating interventions may change based on the amount of time a patient will be homebound. For example, we can work with homebound clients for a short period as they recover from surgery or when discharged from the hospital, but the time they are homebound is finite. Then, there are other clients who are homebound for a more extended period. These clients may be immunocompromised and cannot travel into the community, or they may have a severe physical disability and are functionally bedbound or chairbound and unable to access transportation. These clients may not be able to leave their homes in the near future and so the need to address seating needs in the home is great.
It is essential to determine if the client requires home intervention or would best be served in a specialty clinic. Additionally, we need to consider how long the client will be homebound and their ability to travel to an outpatient clinic. We will talk more about the specialty seating clinics later in this presentation.
Challenges of the Home Environment
Accessibility Barriers
Condition of Home
Weather/Temperature
Clutter
Pets
Pests
People
Distractions
If you have worked in home care, you are probably familiar with many of the challenges that may be found in the home environment. For example, many clients are wheelchair-bound or bedbound and cannot get out of their homes. They may have steps and require the assistance of caregivers to carry them in and out of the house, or they do not have a very accessible home. Many clients live in urban areas where they are confined to one room because their doorways are not wide enough, or they do not have a bedroom or bathroom on their first floor. Often, they may be staying in a living room or dining room. Second, the condition of the home can be a barrier. A house may be in disrepair with uneven floors or walkways that have not been maintained well.
There are also environmental considerations like weather and temperature to consider, particularly during COVID. PPE may make the clinician feel very hot, making it more difficult for both the clinician and the client in hot temperatures. Outside weather conditions like rain, snow, and ice may make it challenging to complete equipment demonstrations or get equipment in and out of the home.
Some of our clients have clutter in the home, making it hard to assess the client. For example, if they work on wheelchair propulsion, they may not have sufficient space to maneuver. We may need to help them identify pathways to travel through the home or help them make a plan to reorganize the space. They may also have pets in the home. The best practice, in my opinion, is that we ask pets to be constrained out of the treatment area, as they can be a distraction. Some people may also have pests or bugs in their homes as well.
There may be other people in the home, which can be positive or negative. People who are not direct stakeholders in the client's care may provide input and ideas during your assessment which can be distracting. However, access to the caregivers invested in the client's care may be beneficial.
Finally, there can be many distractions during certain times of the day such as a preferred television show, kids coming home from school, et cetera. I like to preserve our visit time for us to work together during the session. If I am going to be doing more advanced seating and positioning intervention, I want the client and the caregiver's full attention.
Who Needs a Wheelchair?
Unable to ambulate
Chairbound
Bedbound
Unable to ambulate functionally
Needs assistance
Fatigue
Unsafe/falls
There are two categories of people who need a wheelchair; those unable to ambulate or are bedbound/chairbound, or those who need a wheelchair to mobilize from one point to another.
Individuals unable to ambulate functionally make up the second category. This category is critical to consider because this is an opportunity for intervention. This could be a person who is discharged from an acute or subacute rehabilitation facility, unable to ambulate without assistance, and requires a caregiver available upon discharge. However, they still require assistance and cannot ambulate independently and safely. They may not have sufficient endurance to walk throughout the day or are unsafe and incur falls. This type of client would benefit from having a wheelchair to move from one place to the other in the house without assistance. It also may preserve their endurance and reduce their risk of falling. Perhaps clinicians thought these clients would be independent ambulators at home upon discharge and did not order a wheelchair. However, in the home it becomes clear they will be more functional using a wheelchair.
Benefits of Completing a Seating Assessment in the Home
The clinician has the opportunity to serve clients who are homebound and unable to travel to an outpatient seating clinic.
The clinician can see the client's home environment to address accessibility challenges.
The clinician is able to understand what activities are most meaningful to the client and/or their caregivers.
There are some benefits to completing a seating assessment in the home. One of the most significant benefits is that the clinician has the opportunity to serve clients who are homebound and unable to travel to an outpatient seating clinic. We can see people who otherwise would not have access to service, which is the most powerful point in the presentation. I will provide some case examples that illustrate how important this can be for our clients later on.
The second is that the clinician can see the client's home environment to address accessibility challenges. Many times, there is an insufficient area for the patient to maneuver. We can address those issues and help them problem-solve to make them independent within their home.
Finally, we can interact with the whole family system and understand what activities are the most meaningful to the client and their caregiver(s). We can get a good idea of what the client likes to do and how and where they want to spend their time. A home assessment allows us to make informed decisions about what type of equipment will be the most effective. We can provide ongoing education and training to the client and the caregivers in their own environment.
Mobility-Related Activities of Daily Living (MRADLs)
Toileting
Dressing
Grooming
Bathing
Feeding
*Justification centers on the need for the wheelchair to complete MRADLs in the home
MRADLs are toileting, dressing, grooming, bathing, and feeding. Mobility-related activities of daily living are essential because our justification for any seating and positioning intervention centers on needing the wheelchair to do things like getting to the bathroom, being able to access clothes from the closet to get dressed, being able to get in front of the sink for grooming, being able to get to the tub for bathing, or being able to sit with appropriate trunk support to feed themselves independently and reduce the risk of aspiration. I always include these daily tasks with my seating and positioning interventions.
Case Examples
One case shows a scenario where we are introducing a new seating system, and the other is modifications to an existing seating system. Keep these cases in your mind as we move on to talk about the seating and positioning process.
George
George is an 85-year-old man who lives alone. He was having pain and swelling in his joints and had a fall at home. After the fall, he had so much joint pain that he was bedbound. His family did not want to take George to the hospital, so his primary care provider referred home services. When home health started, George was unable to get out of bed, and his daughters were providing 24-hour care.
George was dependent on care from his daughters. They bathed him, and he used a brief to go to the bathroom. George is an example of someone who is considered fully bedbound. He needs a wheelchair and seating and positioning intervention to be more mobile within his home.
Marlon
Marlon is a 55-year-old referred for home health services. He had a spinal cord injury two years ago, and his ultra-lightweight wheelchair was ordered during acute rehabilitation. In the two years since his injury, he has developed lower extremity contractures and wounds on his lower extremities. The issues with his lower extremities limit his ability to tolerate and propel his wheelchair.
Marlon is an example of someone who received a specialized seating and positioning intervention. Now, he is receiving home health care for his wounds, and his equipment is no longer appropriate for him. We need to look at how we can make modifications and adjustments to achieve his prior level of functioning.
Seating Process
Assessment
Product Trial
Documentation
Funding and Procurement
Delivery and Training
Maintenance
(RESNA, 2011)
According to RESNA, Rehabilitation Engineering and Assistive Technology Society of North America, Seating is a multi-step seating process. We first assess their current functional status. The second is a product trial where we look at how different seating and mobility products meet their needs. There is also documentation where we describe the clinical justification for the equipment, the funding and procurement process, and training after their equipment is delivered. Lastly, we look at the long-term maintenance of their equipment. Even if we do not follow a client along their entire rehab journey, we may see them at different points during the seating and positioning process and therefore need to be well versed in all areas of intervention.
Seating Process: Assessment
Client Assessment
Social history
Medical History
Function
Strength
Range of motion
Tone
Sensation
Cognition
Vision
Body Habitus
The first area of the seating and mobility process is the assessment. We need to assess the client, their environment, and their occupations to develop a profile to help us determine what type of seating system will work best for them. I like to always begin with the client's social history. I want to learn about the client. What do they like to do? Did they work in the past? Do they want to work again? What is their family support system? Do they have any hobbies? How independent are they? How independent have they been in the recent past?
I also like to understand their medical history. What diagnosis do they have that might be leading them to require seating and mobility equipment? What other pertinent medical diagnoses do they have? What is the prognosis of these conditions? It is essential to talk through the medical history with the client in addition to a thorough chart review.
I want to understand their functional abilities, including strength and range of motion in their upper and lower body. I pay particular attention to any range of motion limitations that will impact sitting posture or seated MRADLS. I look at muscle tone to see if they have any spasticity and when it might be elicited or if they have low tone and require additional support in some areas. I need to know if they have intact sensation in their feet, legs, and arms, and any type of sensation impairments they may have for pain, light touch, et cetera.
I am always interested to know the client's cognitive status. I have been in many situations where a client has had significant cognitive impairments that have impacted their ability to use a seating system. In some cases, the team thought they would not be able to access a power wheelchair or be unable to use a power tilt to perform pressure relief, but we were able to address their cognitive limitations and develop some modifications to address these issues.
We also need to understand their visual function. If an individual has low vision or a visual field cut, this can be a significant safety issue for wheelchair propulsion. We might need to do modifications or extensive training. I have had patients with field cuts who could successfully drive a power wheelchair and others who could not.
Finally, I like to make some notes about their body habitus, or any areas where they carry extra weight that may impact their seating and positioning. For example, some clients carry more weight in their lower body, so they may need a wider seat and smaller back support while others may have a broad chest and narrow hips and thighs.
Functional Goals
Participation
Mobility
ADL's
IADL's
Social Interaction
Leisure
What does the patient want to be able to do? This question should be at the center of the whole process. I like to get the caregiver involved, especially when the client is not able to clearly define their goals. I look at their mobility. Do they want to be able to get around their bedroom, house, property, and/or community? The client's functional goals can change some of my decisions. For example, if their goal is to spend a lot of time outdoors, I need to consider that when selecting wheels and tires.
Where will they do their ADLs or MRADLs, and what tasks do they think or want to be independent? What areas of their home do they want to access to complete these tasks?
I also like to know what their IADLs goals are. Do they want to be able to cook or do laundry? Are they caring for children? Do they work at a computer workstation? One of the benefits of being in the home care setting is assessing all of these areas. For example, if they want to do laundry, we can see how they would access that area.
It is also essential to think about social interaction and where this individual or family spends their time? Do they spend most of their time in the living room or the kitchen? Do they have a patio that they like to enjoy, and can the client access that area? Social interconnectedness is crucial, and we must have a plan for the client to access areas where their family members are completing their routines and occupations. I provide education on potential home accessibility modifications throughout the seating process.
Finally, I want to understand what the client's leisure activities are. Do they like to sit and crochet? Do they play computer games? Are they using a cell phone a lot? For this individual, we may need to consider a cell phone mount. I always want to know what a typical day looks like for an individual. Then, I can make sure the seating system that I am recommending addresses all of their occupations and environments.
Postural Assessment
Assess posture in sitting and supine
Identify reducible and non-reducible abnormalities
When I begin a postural assessment, I am not deciding what seating system they need. Instead, I am trying to define what I see, how the client moves, and what type of support is required. I always assess posture in both sitting and supine. I also look at their range of motion, strength, and functional reach. Later, when I get to my product trial, I will pair the client with some potential products based on my observations.
I want to identify reduceable and non-reduceable postural abnormalities. Reduceable is what was previously called flexible, and non-reduceable is what people have referred to as fixed. Seating specialists have moved away from the term "fixed" since the term fixed gives the impression of a static state; however, these limitations can still progress. The term non-reduceable shows that we have identified some postural abnormalities that we cannot correct, but have the potential to get worse.
Challenges of Postural Assessment in the Home Setting
Lack of skilled hands
Solutions: Family, co-treat, vendor
Insufficient support surface
Solutions: Bath bench, transfer board under cushion, firm chair
There are some challenges in the home setting. The first one is a lack of skilled hands. When assessing a client, you often use hands-on assistance to mock up what support they need. In a clinic, a fellow clinician can provide verbal and visual feedback, while a clinician typically treats alone in the home. I have to develop a plan to have another set of hands. Sometimes, a family member can follow instructions to provide that support. Other solutions could be scheduling a co-treat with a colleague or a vendor may be able to assist.
A second issue is that there may not be a sufficient support surface to assess their posture. Many clients are in hospital beds against the wall, and it is difficult to get behind them. Their bed mattress may be soft, and you cannot tell which way their pelvis is going because they are sinking in so deeply. One idea is to use a tub transfer bench as it has a firm surface. You may also be able to use a transfer board under a couch cushion to make the surface more stable. Depending on the patient's trunk balance, you can also use a dining room chair.
Pelvis
The pelvis is the foundation of posture
Obliquity (vertical rotation with right or left side higher)
Rotation (lateral rotation with right or left side anterior to the other)
Anterior/posterior tilt (Anterior tilt the top of the pelvis tips forward promoting lordosis, in posterior, it tips back toward sacral sitting)
I always start with the pelvis (Figure 1).
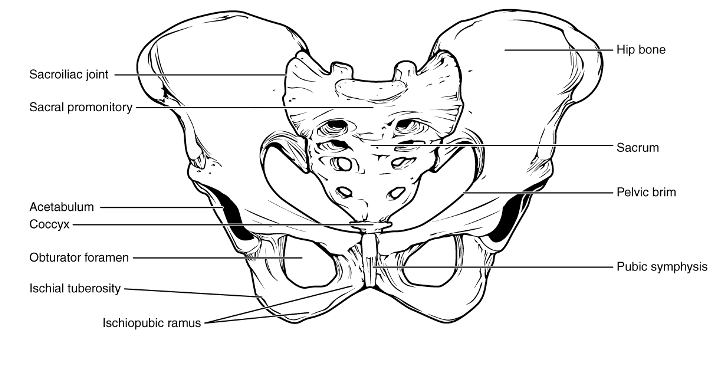
Figure 1. Drawing of the pelvis and labeled with various anatomical locations.
When evaluating the pelvis, I take my two thumbs and place them at the top of the pelvis to see if it is level or lifted higher on one side to indicate a right or left pelvic obliquity (denoted by the person's lower side). Similarly, I see if the pelvic is rotated forward on the right or left side or tilted posteriorly or anteriorly. Sometimes I will put my hands right under their ischial tuberosities to see if there is equal pressure. As I am doing this, I think through strategies to see if I can add some support to bring them into a neutral position or decide if they have restrictions that do not allow a neutral position. If they have flexibility in their pelvis building up under the lower side can provide correction, while we may need to build up under the higher side to accommodate. Again, we want to do this both in sitting and supine. You can then describe the position of their pelvis before you meet with a vendor, as this determines some of the products that you might want to try.
Spinal Assessment
We also want to assess the spine to see any vertebral column issues, as noted in Figure 2.
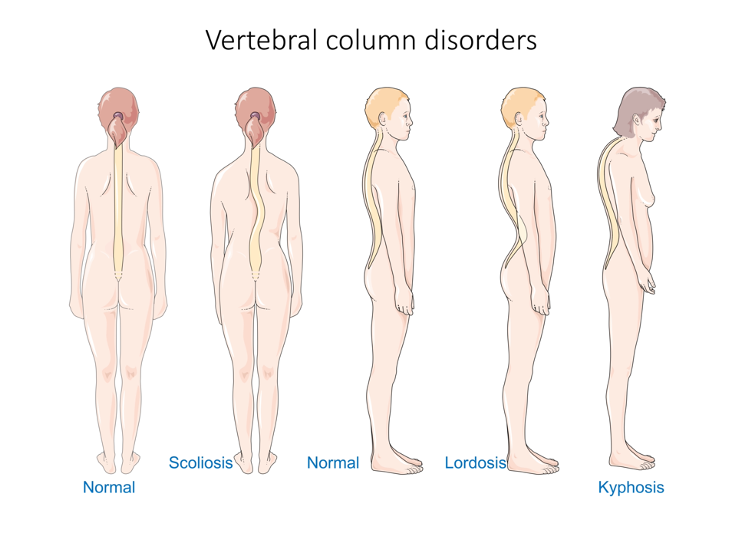
Figure 2. Illustration of different vertebral column disorders including scoliosis, lordosis, and kyphosis.
Ideally, the spine is aligned vertically with normal lumbar and thoracic curves. Our clients can have scoliosis– a lateral curve in the spine. This vertebral column lateral deformity is usually paired with pelvic obliquity. They may also have lordosis, an exaggerated curve of the lower lumbar spine, or kyphosis, an excessive forward curve of the upper spine. Again, we want to define what we are seeing and determine if it is flexible. Can you give them trunk support to get them neutral or reduce the deformity manually? Can you provide them with some trunk support or open up their hip angle to get in a better position? Are they able to have a neutral head position in supine? As I complete my postural assessment, I write this information down to help me formulate a treatment plan later on.
Environmental Assessment
Entry and exit
Access to key areas
Bedroom
Bathroom
Preferred areas
Meals
Social activities and shared spaces
Leisure and outdoor spaces
Community
Finally, I look at their environment. How is the client going to get in and out of the house? Do they have a ramp? Will they be relying on someone to carry them? Can they walk up and down a step with assistance, or will they be bumped up and down in their wheelchair? Do they have an uneven walkway? How wide are the doorways?
I start with critical areas like their bedroom and bathroom. Then I look at their preferred locations in their home. Where do they take their meals, and where do they want to take them? What are the social activities and shared spaces? Are there outdoor spaces they want to be able to access? Where might they want to go in the community?
Some clients have reliable, accessible transportation, whereas others do not. Clients who live in urban areas may go out their door and around the corner to a mini-market. This is part of their immediate environment that they plan to use. We need to understand their goals for these types of environments.
Accessibility
Americans with Disabilities Act (ADA) Guidelines (www.ADA.gov)
Local codes and regulations
Regardless of standards, accessibility is dependent on the size of the wheelchair.
For accessibility, there is a lot of information under the ADA, and there are also many local codes and regulations that we need to follow. If you have specific questions, I recommend that you look at ADA guidelines. Regardless of standards, when we are in the home, accessibility will depend on the size of the wheelchair compared to the size of the space.
For example, I recently did a home assessment. The client lived in a first-floor apartment. The home was ideal as it had a bathroom on the first floor with a straight path to pull right in. There was also an accessible level entry and a wide berth for turning in the hallway to access the bedroom. The only problem was that this was a bariatric client that weighed over 400 pounds. Based on the size of his wheelchair, he was not able to access those areas in his home. For residential construction, everything looked pretty good, but it was not going to be accessible for this client. Thus, you need to know the size of your client's equipment.
Seating Process: Product Trial
Product Trial
When possible, it is desirable for the client to have the opportunity to trial products being considered for their seating system.
When a trial of the exact products is not possible, a simulation may be used.
Product trial determines if the seating system will meet the user's needs and verify it can be used safely.
In the product trial, we are taking all of the information that we gained in our assessment and thinking about what type of wheelchair and seating system a client may need. When possible, the client should try the exact products being considered, and hopefully, the vendor is able to bring what you need. This is one of the challenges of working in the home setting. In contrast, when I worked in an extensive rehabilitation hospital, I had a whole closet full of backs, cushions, and wheelchairs. I could try different equipment, and if something did not work, I could switch it out.
As everything has to be brought into the home, this is something to think about when doing your assessment. Can you get the products that you need to trial with the client? This is something to keep in mind when deciding what patients are appropriate for a home seating assessment. Providing the vendor with a good description of the postural assessment ahead of time and discussing the types of supports that are needed will allow the vendor to have appropriate demo equipment in the home.
When possible, it is desirable for the client to have the opportunity to trial the exact products being considered for their seating system. When a trial of the same products is not possible, a simulation may be used. For example, if you think the client needs a lateral, but you do not have a lateral, you may position your hand to determine where the support is required. Although it is not ideal, you may not have a choice.
A product trial determines if the seating system will meet the user's needs and verifies if they can use it safely and are not a risk for falls or a pressure injury. Documenting the results of the product trial in terms of function is an important part of documentation. In the recommended equipment, can the client reach to their face, reach forward to their environment, propel, perform pressure relief? What is their sitting tolerance and propulsion distance and speed?
Equipment
Durable Medical Equipment
Complex Rehabilitation Technology (CRT)*
There are two different terms that you may hear in reference to equipment. The first is durable medical equipment or DME. The second category is complex rehabilitation technology or CRT. CRT requires an assessment by a physical or occupational therapist, and it requires the presence of an ATP order. In the slides below, I am going to review wheelchair bases. I have starred the term CRT to help you identify what equipment can be ordered without an assessment and what equipment cannot.
Manual Wheelchairs
Let's first look at manual wheelchairs. Figure 3 shows a comparison between the different options.
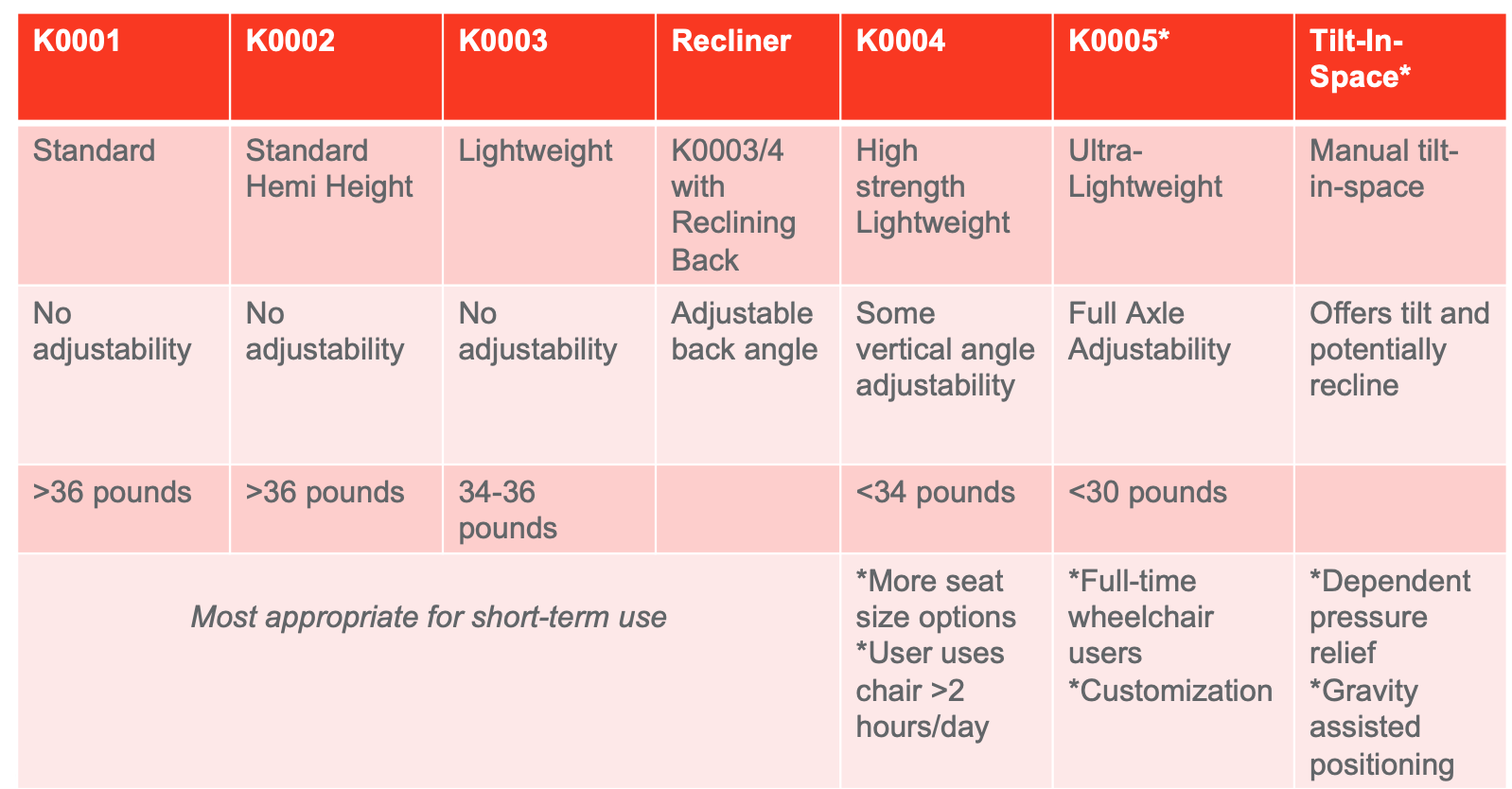
Figure 3. Chart defining components of different manual bases.
You need to justify the most appropriate equipment for your client. For example, I may start with a K0005, and if I cannot explain that wheelchair base, I then move down to the K4. We want our clients to be independent, safe, functional, and not have shoulder strain and need to look at the client's diagnosis, function, or body habitus to do so. You can also ask your vendor about the components you need to justify.
To start, I am going to talk to you about the types of manual wheelchairs.
The first is a K1, and this is a standard wheelchair frame that is heavy and has no adjustability.
A K2 is a standard hemi-height wheelchair with a lower seat to floor height.
K3 is a lightweight wheelchair, but it has no adjustability. The weight of the K3 frame is about 34 to 36 pounds and is most appropriate for short-term use, perhaps for someone recovering after surgery. A recliner is usually a K3 or K4 category with an adjustable back angle. As a permanent solution, a recliner wheelchair is typically not appropriate; however, it can be used in some situations where the client needs an open seat to back angle without adjustment or postural support. For example, it can be an appropriate option for some post-surgical clients who need their legs in extension.
K4 is a high-strength lightweight wheelchair. This has some angle adjustability, weighs under 34 pounds, and has more seat size options. K4 frames are for users who will be up in their wheelchair for greater than two hours a day.
Someone who will be a day-to-day wheelchair user needs to either be in a K4 or a K5 frame. A K5 frame is considered complex rehabilitation technology. It is an ultra-lightweight wheelchair, has full angle adjustability (up and down, front and back), and has the option for camber. Camber is angling the wheels toward the frame to improve turning ability. The K5 frame weight is much lower than other options at below 30 pounds and is for full-time, active wheelchair users like a young client who will be doing wheelies to access curb cuts in the community.
If we have an active wheelchair user, are we going to do their seating evaluation in the home health setting? It depends. If they are very active, they may not be homebound. However, we do have some people who benefit from a K5 frame who are homebound. This can be an excellent opportunity to do a product trial. You bring in a frame to see where the axle might work the best and look at some of those different features.
Finally, under manual wheelchairs, we have tilt-in-space bases. There are some options for a power tilt on a manual chair. There is also the potential to have recline on a manual tilt-in-space to have both tilt and recline. Tilt-in-space is for dependent pressure relief. Most likely, caregivers will be providing the client's pressure relief unless they have insurance and there is justification for a power tilt. Tilt is also an excellent option for a client who requires gravity-assisted positioning. They may have trouble maintaining an upright position, and tilting them slightly brings them into a better position and provides rest breaks without gravity. This is another justification for a tilt-in-space wheelchair.
Power Wheelchairs (PWC)
I have outlined four different types of power wheelchairs in Figure 4.

Figure 4. Chart comparing the different types of power wheelchairs.
There is also a Group 4 power wheelchair, but as this is more advanced equipment and not typically covered by insurance, I am considering this outside the scope of this talk. Scooters offer minimal postural support, and they do not have any ability to reposition the patient electronically. It is also rare to have a client who has space for a scooter in their home. If you have a vendor bringing out equipment for a product trial, you can quickly identify if the client can use the scooter within their home and if the equipment can help with mobility-related ADLs like getting to the bathroom.
Group 1 power wheelchairs have basic seating and offer minimal postural support or seat functions. They have lower battery life and are for patients with no postural abnormalities, pressure injury risks, and need it for only moderate distances like within the home or grocery store. Group 2 power wheelchairs typically have captain seating, but some rehab seating options are available if you think your client needs a specialty cushion or back. They may also have one seat function like tilt. Group 2 power wheelchairs have a more durable base with longer battery life and are for all-day users. Then finally, we have the Group 3 power chairs with integrated rehab seating. This is where we build custom seating systems.
Power Seat Functions
Tilt
Recline
Leg elevation
Seat elevation
Power wheelchairs can have up to three or more seating functions. These power seat functions are specifically designed for clients with neurological conditions like myopathy, congenital skeletal deformities, et cetera. It also has better drive wheel suspension. For example, if you have a client with spasticity and bumping makes them spasm, this can be controlled better via a more advanced drive wheel suspension.
There are also alternative drive methods such as a head array or a sip and puff. If this type of driving method is required, they need a Group 3 power chair for the upgraded electronic capability. Power seat functions on a Group 3 power wheelchair include tilt, which is the wheelchair tilting fully with the seat and the back moving together, recline, where only the back moves, and leg elevation, where they can elevate their legs. There is an option for combined recline with leg elevation for clients who need to be in a supine position for assistance with hygiene like a female catheterization. Lastly, there is seat elevation, which is the ability to elevate the seat. This option can be great for a client to move up to eye level with peers during social situations or for accessing items from cabinets. However, it is a complex item to justify through insurance and is typically an out-of-pocket expense.
Power Assist
Provides battery-powered assist to propel a manual wheelchair
A power assist is a battery-powered option to help propel a manual wheelchair. It can either be embedded in the wheels or attached to the bottom of the wheelchair. It provides extra power to manual wheelchair users with decreased endurance or who require an extra boost in different circumstances like inclines.
Seating and Positioning Components
Backrest
Cushion
Headrest
Arm Supports
Leg Rests and Foot Supports
Pelvic Positioning Belt
And more!
After establishing the appropriate base for them, we look at the seating and positioning components. This is not an exhaustive list, but these are the things to consider. What backrests do they need? What cushion do they need? What headrest would be helpful for them? What other supports are required? You need to identify what components will provide a functional position for your client.
Pelvic Position is Primary in Positioning
Address pelvic positioning prior to developing other interventions because poor pelvic positioning may make other components appear incorrect.
For example, if the pelvis is too far forward in the wheelchair…
The seat depth will seem too short
The leg rests will seem to short
The headrests will seem too high
The pelvic positioning belt will seem too tight
We always need to start with the pelvis prior to developing other interventions because poor pelvic positioning may make other components appear incorrect. For example, if the pelvis is too far forward in the wheelchair due to inadequate support or sliding forward into a posterior pelvic tilt, the client's seat depth and leg rest position will appear too short. Their knees and headrest will seem too high. In fact, the headrest will be over their head. They may feel like they cannot focus or their seatbelt is too tight. Before you loosen the seatbelt, you have to make sure that they are correctly positioned in the chair. Often, we need to teach the family not to move the headrest as it was initially set at the right height. Instead, they need to make sure their loved one is sitting correctly. You do not want caregivers or staff to adjust the equipment components like the headrest, legrests, seatbelt, or add in pillows. Instead, they need to be trained to pull the client back into their seating in an excellent pelvic position.
Wheelchair Cushions
Materials
Foam
Gel
Air
Incontinence Cover
Solid Seat Insert
Types
General Use
Skin Protection
Positioning
Positioning and skin Protection
Custom and adjustable options
There are many different types of wheelchair cushions made of different materials that I will review. You also need to have a conversation with your vendor about what you can justify for your client. Criteria may include skin protection, positioning, or both positioning and skin protection. Custom and adjustable options might be best managed in a specialty seating clinic, but occasionally we may need to do it in the home. You want to be able to justify the one that is most appropriate and best for your client.
The first type of material is foam. Foam is lightweight, but if it does not have a cover, especially for clients with incontinence, this can become an issue. A gel cushion is also suitable for pressure relief, but it can be hot if you have a very sweaty client and can create a moist environment. For a client with incontinence, sweaty, or a history of yeast or fungal infections in the groin, you may want to do a little bit of a more extended product trial to make sure you order the most appropriate material. Finally, there are air cushions. Air is excellent because it is lightweight, but it does not have the same support that you might get out of a foam option. Air cushions need to be refilled periodically and monitored for the correct amount of air. And, if the client and/or caregiver are not very careful, it can be popped. You also need to be very cautious when you have a client who does not have good sensation or is insensate because they may not feel that they are bottoming out on a low air cushion. I am very selective when I use air cushions, but it is an excellent strategy for those with skin breakdown if it can be monitored appropriately. Again, if the client has incontinence, I always have a conversation with the vendor to see what options would work best like an incontinence cover.
For a wheelchair with a sling seat, you may need to add a solid seat insert to provide more stability. This also improves the efficiency of propulsion, whether with their arms or feet.
Pressure mapping might be an option to assess the efficacy of a specific cushion or for a client with skin breakdown. This mapping shows how the pressure is distributed over a cushion and can be great technology if you are not sure what the best solution will be for your client.
Back Supports
General Use
Positioning- Posterior
Positioning- Posterior and Lateral
Custom Fabricated
Planar with Lateral Supports
There are many different back supports depending upon your patients' needs. Do they need a general use type back or more of a custom back that provides posterior and lateral support? Can they use a flat back or something with curves to align with the body? It will depend on what will help the client have the best functional position.
Basic Seating Principles
Identify what equipment is medically necessary.
Accommodate non-reducible/fixed postural abnormalities
Address reducible/flexible postural abnormalities
Use least restrictive options
Work Posterior>Lateral>Anterior
Monitor function, comfort, and skin integrity with all interventions
You also need to know what is medically necessary and justifiable for the client. What diagnosis and impairments do they have, and how can this equipment meet those needs? If there are non-reducible fixed posture abnormalities, how will we accommodate that? If there is a flexible deformity, can the equipment be used to get them in a neutral position? Overall, the seating system needs to address their needs and provide a neutral, functional position.
You always want to use the least restrictive options. I was trained to start in the posterior. For instance, you can start with a backrest, and if this does not work, then you can perhaps add some laterals. As a last resort, we add anterior support like a chest strap. You are always looking to develop back support through a posterior or posterior and lateral approach. This is the same thing with a headrest. You start posteriorly, add additional lateral support if needed, and add anterior support only as your last option.
We want to monitor their function, comfort, and skin integrity with our interventions. I have had clients where I came up with a seating system that I thought was fantastic but did not work for the client. It could be that the comfort was not there, or it was difficult for them to function in the prescribed equipment. And, sometimes, clients are not always able to communicate that. This is why a product trial is so important to see if it works for them.
I will talk more about skin integrity in a moment, but I think it is so important that whenever we are changing anything in a client's seating system, we need to teach them to monitor their skin. Thus, if we change their position or equipment, they need to watch their skin. Is there any red on their bony prominences, or does their skin look different?
Common Seating Interventions
Falling to Side
Address pelvic obliquity
Add lateral trunk supports
Hunching Forward
Open back angle
Add lumbar support
Sliding Forward
Add thigh support/seat depth
Provide foot support
Add seat slope
Evaluate hamstring length and consider removing elevating legrests
Add or change the position of the pelvic positioning belt
Legs Falling Out to Sides
Add seat depth
Add lateral thigh support- thigh guide or cushion build-up
Unable to Complete Functional Reach
Add trunk support (lateral support, open back angle, seat slope)
Falling to the side. These are some things you might see and some ideas of how you might approach these issues. The first scenario is a client that is falling over to the side. We may need to provide lateral trunk support or address a pelvic obliquity. If we need to reduce a pelvic obliquity to neutral, we may build up the lower side of the pelvis to bring it to neutral. If we cannot move the pelvis to neutral, we will have to accommodate the high side of the pelvis. I always look at this carefully with my vendor. In this situation, I may also pursue pressure mapping to ensure there is not too much pressure on one side versus the other.
Hunching. Sometimes you have a client who sits fine in their wheelchair, but they start to fall as soon as they lift their arms. This can signify that they need more lateral support or have insufficient lumbar support. Opening up the wheelchair's back angle can allow gravity to help them maintain a more upright posture. When they have a more upright posture and line of sight, they have much access to the environment and social interaction.
Sliding forward. You may also see a client that slides forward in their wheelchair. We may add thigh support or increase their seat depth. More support under their thighs allows more offloading of their ischium and provides better pressure distribution and comfort. Perhaps they need a different cushion to be more comfortable. Their footrests may be too low, and they may be sliding forward to try and get their feet down to the footrest. Sometimes, it is simple, like making a minor pin adjustment in the footrest, adjusting the back angle to help gravity keep them back in the chair, or adding seat slope. They may not have sufficient hamstring length, so when they stretch their legs out, it pushes their pelvis into a posterior tilt and then causes them to slide forward. Hamstring length with elevating leg rests is a very important thing to consider. Lastly, they may just move around quite a bit and need a pelvic positioning belt to keep them back in the wheelchair. I had a client who fell out of his wheelchair because he thought he had his seatbelt on and did not. He was reaching behind the wheelchair and slid right out the front. A pelvic positioning belt can be necessary for dynamic activities, especially if the client is propelling or foot propelling, to keep them in the wheelchair and prevent forward sliding.
Legs falling out to the side. If a client's legs are falling out to the side, this may be because the leg rests too high or the seat depth is too short, and they are not getting support under their femurs. Lateral thigh support can be added either within the cushion or with a thigh guide attached to the side of the wheelchair.
Unable to complete functional reach. Finally, if they cannot complete functional reach, we can add trunk supports, open the back angle, or add a slope to the seat cushion.
The Product Trial Includes Functional Tasks
MRADLs
Propulsion
Pressure Relief
Functional Reach
Make sure you look at how the client does dynamic activities within the wheelchair. What are the things that the client wants to do during the day? Can they maintain their position while they are eating? If they cannot, they are not in the right seating system. The client should not be working to sit upright in their chair. Sitting should be a more passive posture, not exercise. We should develop a seating system that provides them the support they need to do the things they want and need to do. If they want to exercise, they can go to the gym or do their home exercise program.
You want to see how they are doing their mobility-related ADLs. How are they propelling? How are they doing their pressure relief? How are they reaching into space? Can they get to all their workspaces? The product trial needs to be more than a few minutes to allow the client to weigh in on these things. You may need to negotiate with the vendor so that the client keeps the equipment long enough to ensure that it meets their needs.
Home Accessibility Considerations
Seat Width
Leg Rest Type
Wheel Size and Hand Rims
We also need to look at home accessibility considerations. A client may fit into an 18 or 19-inch seat width, but ultimately, the wheelchair width may depend upon their door widths. What is their seat width going to impact? This is also the same thing with their leg rest type. Elevating leg rests can make their wheelchair base long and make it difficult to turn within their homes. We also want to look at wheel size and hand rims. Larger wheels create a larger turning radius. We need to be cognizant about what will be most functional in their space. For example, there are situations where omitting the hand rims can get you that last half-inch that you need to avoid any structural home modifications. Although it is not ideal, it may be the only viable solution, especially for a client who is dependent on propulsion. During the product trial, you can see if they can get the wheelchair into the bathroom, bedroom, or wherever they need.
Seating Process: Documentation
Documentation-Therapist
Provide medical history and seating diagnosis
Clearly state why a wheelchair is needed
For example, the client is unable to walk
Consider objective measures
Clearly list all desired components with a justification for each
State why other options are not feasible
Cross-reference with supplier's order form
Add how this component promotes function or reduces the risk of a secondary complication
If items are replacement items, document why the existing seating system does not meet users' needs.
My documentation starts with a postural assessment. I want to provide a medical history and a seating diagnosis. Why do they need a wheelchair? For some CRT, the client may need to have a neurologic diagnosis related to their seating needs. You need to make sure you do a chart review to look at everything. It might not be a diagnosis of stroke but a diagnosis of hemiplegia that helps with the justification. You also want to quantify their function and talk with the vendor about the seating diagnosis that is most appropriate for the equipment that your client needs.
You need to clearly state why a wheelchair is required– for example your client cannot walk. While something may seem obvious to you, the review team has never seen your client. We need to spell it out. You also want to use objective measures like their ADL status, fatigue, time out of bed, fall risk, et cetera. You need to quantify outcomes if you can. How does the seating system that you are recommending change their functional outcomes?
We want to list all of the desired components and justify each one while noting why lesser options are not feasible. For example, why does a client need a power wheelchair and not a manual wheelchair? Perhaps, they cannot propel a manual wheelchair. We need to expressly state that. Why does a client need a custom back and not a slingback? They need postural support. When you develop an order with a vendor, you can ask them for a form and go line by line for each item. This is an excellent way to identify the documentation that you need.
If you are doing replacement items or wheelchair modifications, you need to document why the existing seating system does not meet users' needs. For instance, I talked earlier about the client whose leg position had changed, and he could no longer use his leg rests. He had even done some foot propulsion before. We had to modify the floor to seat height and justify why he needed different legrests and tires. This was all because his propulsion mode had changed. Before when he had foot-propelled, he did not require a tire with a lot of tread, but now, he needed tread on the tire to be able to get around his home. You need to describe this to the reviewer.
Documentation-Provider
Patient must have a "face to face" visit with provider for wheelchair prescription
Mobility evaluation must be the purpose of the visit
Documentation should include:
Height, weight
Mobility-related diagnosis
Objective quantification of strength and mobility
Functional need for wheelchair
Provider will sign off on the therapist's documentation.
(Michael et al., 2020)
We also need documentation from a provider. The client must have a face-to-face visit with the provider for a wheelchair prescription. Some DME can be ordered by the provider directly without a therapist order. You may collaborate with the provider and have them put in an order for you. I worked with a client who needed a wheelchair and "spec'd" out a K4 wheelchair, including the specific components that I thought she needed. Her provider put the order in with the DME vendor because they were familiar with that particular vendor. So, we were able to collaborate and get the equipment that way. However, for CRT, the mobility evaluation must be the purpose of the visit. The documentation from the provider should include the height, weight, mobility-related diagnosis, and objective quantification of strength and mobility. If the therapist generates the letter of medical necessity, the provider will sign off on the therapist's documentation.
7 Element Prescription
Client name
Description of the item ordered (power wheelchair, manual wheelchair, scooter)
Date of completion
Pertinent Diagnosis/Conditions
Length of need
Physician Signature
Date of face to face evaluation
Medicare will often require a seven-element prescription, but this is also good to keep in mind for your wheelchair documentation. The prescription needs to have the client's name, the description of the item ordered, the date of their assessment completion, pertinent diagnosis and conditions, length of time that they think the client will need the equipment, physician's signature, and have the date of the face-to-face evaluation.
One final thing I will say about the documentation is that if you feel overwhelmed about how to quantify your postural assessment and the recommended equipment, some vendors can provide a template for you. There are also templates available online. You can also go to the RESNA website because they have some great information on how to construct a letter of medical necessity. Or, if you are a professional association member, there may also be resources there. You do not have to invent everything for yourself.
Seating Process: Funding and Procurement
The vendor will submit for insurance approval.
Once funding is approved, the vendor will order the seating and positioning components.
This process can be lengthy. Many vendors have processes to keep clients informed.
Delivery will be scheduled when the vendor has received all components.
After you and the provider create your documentation, you move into the funding and procurement piece. The vendor will submit for insurance approval. Once the funding is approved, the vendor will order the seating and positioning components. Remember, this process can be lengthy, from several weeks to even months. Many vendors have processes to keep the client informed, which is great because you are not operating the phone all the time. It is essential to inform the clients of the process, especially those who are anxious about their equipment. Make sure you have a good strategy for communication. In summary, the vendor receives the funding, they order the equipment, and once they get everything they need to put that seating system together, they will schedule delivery.
Seating Process: Delivery and Training
I love when I can be present for the delivery. I can make sure everything fits and initiate training.
Delivery and Training
The client requires education on how to use and maintain their equipment once it is delivered.
Because of the time from seating clinic to delivery, the client may no longer be on home health services.
Consider requesting a new referral for wheelchair training when equipment is delivered.
For training, the client requires education on how to use and maintain the equipment. If you are working within a certain certification period or have met your other goals and have discharged the patient, they may no longer be on home health services. In these instances, I urge you to request a new referral for wheelchair training when the equipment is delivered. This training can make a difference because if the client does not learn how to use the equipment appropriately, they will not be able to use it effectively or get the full benefit. They might even abandon some of the pieces or seating components.
Positioning
The patient and caregivers should understand how to position the patient properly in the wheelchair.
Folding and unfolding the wheelchair.
Removing and replacing removable items.
Setting-up positioning components.
The patient and the caregivers should understand how to position the patient properly in the wheelchair. They should understand how to fold and unfold the wheelchair if they will store it in a closet or put it in the car. And, if there are pieces that are removable, like arm and leg rests or cushions, you want to make sure that they are comfortable removing and replacing all those items. Have them teach those steps back to you. For example, they may need to move a headrest out of the way to use a Hoyer lift. If so, make sure they can replace it after the transfer is completed.
Pressure Relief
The client/caregivers should be able to demonstrate appropriate methods for pressure relief.
Lateral lean
Forward lean
Wheelchair pushup (potential for shoulder strain)
Dependent tilt
Guidelines for pressure relief vary, and each client has their own skin tolerance.
Commonly 30-90 seconds every 15-30 minutes
Pressure relief is a crucial point of training. The client and caregivers should be able to understand appropriate methods for pressure relief. Suppose you are working with a vendor to do a pressure map. In that case, this is an excellent opportunity to practice pressure relief and show the client how they can unload themselves appropriately. This may entail a lateral lean where they lean to one side and then the other. They may be able to lean forward enough to unload their ischium. Another option is a wheelchair pushup; however, I am hesitant to teach wheelchair pushups as my primary pressure relief method because it puts so much strain on the shoulder. And, if the client is a full-time wheelchair user, they already are at risk for stress on their shoulders. They can also use a power tilt where they or a caregiver tilts them back, making sure they relieve pressure. The caregiver needs to know the proper way to tilt them, even as simple as raising them slowly upright after the weight shift is over.
Guidelines for pressure relief can vary based on the client's skin tolerance. Commonly, what is recommended is weight shifting for 30 to 90 seconds every 15 to 30 minutes for clients performing manual pressure relief. For less mobile clients completing a tilt pressure relief may be recommended at 5 minutes every 30 or 2 minutes every 15. You will probably train the clients to complete pressure relief frequently and then increase the range if their skin is tolerating it well. If the client's skin looks consistently good, they might be able to move that out a little more. It is vital to make sure that you are teaching them how to do pressure relief and monitoring their skin integrity to ensure that they are not having any pressure injuries or skin breakdown.
Transfers
Wheelchair training may overlook functional transfer techniques.
Consider number and type of transfers (bed, commode, chair, car).
Good transfer technique is essential for preventing falls and upper limb injuries.
Poor transfer techniques can have psychosocial consequences.
Four components of transfers:
Technique
Confidence
Balance
Strength
Consider the use of transfer boards as a tool for improved transfer success.
(Barbereschi & Holloway, 2020)
When doing wheelchair training, we often forget about practicing transferring in and out of the wheelchair. When prescribing equipment, we need to consider the number and type of transfers per day and what effect it will have on their overall endurance. And, where are they transferring? Are they going to get into bed, onto the commode, into a different chair, their couch, or in and out of the car? We need to show the client how to set up those transfers to do them safely. Using good transfer techniques is essential for preventing falls and preventing upper limb injuries. Poor transfer techniques can not only cause injuries like falls and upper limb injuries, but they can also have psychosocial consequences. If the client is not confident, they will not get out of their wheelchair. And, if they do not feel comfortable getting in and out of the car, they may not accept an invitation to go to dinner with a friend or go somewhere with their spouse. It may also decrease their confidence overall.
There are four components of an effective transfer. The first one is the technique. How is the client doing the technique? Do they have mastery of the head over the hips relationship? Are they setting up everything properly? Do they clear the path? Are they placing their wheelchair in the appropriate orientation and getting the armrest out of the way? The second component is their confidence. You want them to feel confident that they can transfer well to build their confidence. The third is balance. One of my mentors said, "If the client can't sit and lift their hands off the edge of their seating surface, they are not ready to work on transfers." We need them to work on unsupported trunk balance as a transfer prerequisite. The last component is strength. Do they have the power that they need to lift their body? If they are doing a lateral transfer, are we working on scapular strength so they have the stability that they need to lift and complete the transfer?
Many people do not like to use the transfer board because they see it as a crutch or one more thing to carry around. However, for a client who is not entirely safe or independent, we should not overlook the transfer board as a tool for improved success. This aid can make or break a client's independence, even for clients taking weight through their feet.
Best Practices for Wheelchair Skill Training
Training should be ongoing.
Offer opportunities to practice learned skills prior to introducing new skills.
Customize pace and goals to the client.
A systematic review found that a formal manual wheelchair skills training program improved wheelchair skills in the short term. Still, long-term benefits for manual wheelchair users and uses for power wheelchair users are unclear (Tu et al., 2017).
Training should be ongoing, and we should offer opportunities to practice learned skills prior to introducing new skills. In a moment, I am going to talk to you about a wheelchair training hierarchy; however, we should customize and pace our goals to the clients' abilities. Not every client wants to use their wheelchair outside of their home. Some clients will progress slowly and may need a lot of time to work on specific skills like using wheel locks, while others may only need 10 seconds to master a concept before moving on to the next thing. We are always going to tailor it to the patient.
A systematic review found that more manual wheelchair skills training improved wheelchair skills in the short term, but long-term benefits for manual and power wheelchair users were unclear. Thus, a formal approach to wheelchair training in the short term might be helpful. As long as they get skilled therapy, they are likely to have success.
Manual Wheelchair Skill Training- Indoor Skills
Parts management (brakes, armrests, legrests)
Rolling (forward and backward)
Turning (in place, while rolling forward/backward)
Doors and doorways
Object retrieval (floor, high)
Thresholds
Transfers
(Best et al., 2005)
For manual wheelchair skills training, we start with indoor skills like parts management. Examples are locking and unlocking brakes, flipping back the armrests and replacing, and taking on and off the leg rests. For some clients, this might be an entire session. Then, we look at pushing it forward and backward. Once they are good with this, they can move on to turning. Can they turn while they are rolling forward? Can they turn while they are rolling backward? Can they make a 360-degree turn? Next, we can have them open doors, go through doorways, retrieve items from the floor or a high surface, and go over thresholds. Finally, we can look at all the specific transfers they need to complete.
Manual Wheelchair Skill Training- Outdoor Skills
Crossing the street
Gravel
Incline (ascend, descend, cross slope)
Small Curbs
Potholes
Folding and Unfolding Wheelchair
Car Transfers
(Best et al., 2005)
Looking at a hierarchy of outdoor skills, we can assess how they cross the street, travel over gravel, go up and down an incline, or cross a slope. We can start with a very flat incline and move to steeper inclines, small curbs, and navigating potholes. Can they fold and unfold their wheelchair and complete car transfers?
Manual Wheelchair Training- Advanced Skills
Wheelies
Large curbs
(Best et al., 2005)
There are more advanced skills like wheelies and large curbs. These are not skills that every client will need. And, if you want to work on these skills with a client, you will probably want to look up some advanced training or mentorship in this area.
Power Wheelchair Skill Training
Power wheelchairs can significantly improve independence but can pose safety concerns.
Training should be graded. Skills that are demonstrated in the rehabilitation setting may not translate to home.
PWC Operation: On/Off, speed control, seat functions
Driving: slow to fast
Driving: straight to turning/obstacle negotiation
Driving: open spaces to more confined spaces
Driving: flat terrain to uneven terrain
(Bigras et al., 2020)
For power wheelchair skill training, we start slow and then move into more advanced skills. Power wheelchairs can improve independence, but they pose significant safety concerns. It is imperative that your client understands that the power wheelchair is heavy and has a lot of force. If they drive over someone's foot, they will hurt them. Or, if they hit a doorframe, this might cause damage. This is something to consider, especially in homes with small children or pets.
Training should be graded, and the patient's skills in rehab may not translate to the home. The client is driving through wide hallways and doorways in a rehabilitation hospital. These hallways are typically well lit, and the floors are smooth. When we go into a home, it is good to start back at the beginning. We want to see that they can turn on and off their chair, control the speed, and switch modes to access their seating functions. Can they access all seating functions and switch from function to function? I recently worked with a client that had a power wheelchair, but their family was pushing it because they felt so nervous about the client's ability to drive the wheelchair safely, given their space concerns. We had to go back and work on driving, even showing them how to get the speed down.
Start low, slow, and then progress to faster driving. Driving should start in a vast, open space and then move into turning or obstacle negotiation within a confined space. Additionally, driving should start on flat terrain and move to more uneven terrain. I always want my client to succeed before I move on to more advanced skills. And, in each session, I like to go back and look at the skills they learned before advancing to higher-level skills.
Preparing for the Elements
Protect power wheelchair electronics
Keeping the user dry
Safety in snow and ice
Protect home from dirty wheelchair tires
The other thing I like to think about as part of my training is how to prepare for the elements. Again, in a rehabilitation hospital, the client is probably not going outside in the rain or dealing with snow. Addressing how the client will be using their wheelchair across four seasons can be an essential part of our training, and this will be different depending on the location.
First, you want them to have a plan for protecting the power wheelchair electronics. If they are going out in the rain, is the client holding an umbrella? Where does that umbrella need to be? Sometimes vendors recommend putting a plastic bag over the joystick. We also need to consider how the user will stay dry? If they are pushing a manual wheelchair, they probably cannot hold an umbrella. Are they going to wear a poncho or raincoat that covers their wheelchair? They may be able to attach an umbrella to their wheelchair.
A wheelchair can slip on ice and snow. They may need to take it a little more slowly or avoid going out. They should have a good plan for snow removal for sidewalks and entrances. They will also want to protect their home from dirty wheelchair tires. They may live rurally or have a property with a lot of mud or travel in the city with a lot of salt. All of these can accumulate on the tires. They may need to have a station in the entryway with a nappy rug, stiff brush, towel, et cetera to rid the wheelchair of the debris before going into the home.
Maintenance
Finally, we will talk about maintenance.
Wheelchair Repairs
In a sample of 533 wheelchair users with spinal cord injury, 301 reported wheelchair repairs over the previous 6 month period. Of these, 127 experienced an adverse consequence related to the repair.
Less repairs required in the first year of use.
Active users required more repairs.
Most common repairs: Tires, controller (PWC), positioning supports, battery (PWC), cushion, and seat function (PWC).
Most common adverse consequences: Being forced to use a backup chair, being stranded at home.
(Worobey et al., 2021)
Wheelchair repairs are an unfortunate and challenging part of being a wheelchair user. The research gives you a good idea of some of the challenges that our clients who are using wheelchairs may face. In a sample of 533 users with spinal cord injury, 301 reported requiring wheelchair repairs over the previous six-month period. And, 127 experienced an adverse consequence related to the repair. Fewer repairs were needed in the first year of use. This seems pretty obvious, but what is not so obvious is that even in that second year, those users required the same amount of repairs as people with additional years on their wheelchairs. I believe the range of wheelchair use in the study was two to six years. Thus, the people with a wheelchair that was two years old required repairs at the same rate as someone with a wheelchair that was five years old.
The fact that active users required more repairs does not surprise me as there is a lot more strain on the wheelchair if they are going over different terrain, doing wheelies, and all of those things. The most common wheelchair repairs were tires, power wheelchair controllers, positioning supports (like laterals or thigh guides), batteries, cushions, or power seat functions.
The most common adverse consequences were being forced to use a backup chair or being stranded at home. In a worst-case scenario, a client could be bedbound if not in a wheelchair. It is wise for clients to have a backup if they rely on a wheelchair, particularly for some of these more complex power wheelchairs. Asking the question, "What's your plan for repair?" should be part of our maintenance training.
Wheelchair Maintenance
Clean wheelchair regularly
Rag with mild detergent, stiff brush for debris
Inspect wheelchair regularly
Check brakes weekly
Check tire pressure and tires monthly
Check moving parts and nuts and bolts
Store in a climate-controlled area out of direct sunlight
Schedule annual maintenance visits with vendor
Clients need to clean their wheelchairs regularly. The wheelchair is part of how a client presents to the world, just like bathing or wearing nice clothes. They can take a rag with a mild detergent and wipe it down. A stiffer brush can be used to get rid of debris. I worked with a younger, good-looking guy that was image-conscious, but his wheelchair was very dirty. When I asked him about it, he said that he never really thought about it as he did not get this information during his training. He was so appreciative because he wanted to present a good image.
Clients also need to inspect the wheelchair regularly. They may need to check brakes frequently (every week) and proactively instead of when they are not working well to prevent falls. Brakes may need to be tightened or bolts replaced. Air pressure in pneumatic tires, in addition to other components, needs to be checked regularly. If the client is not a full-time wheelchair user, they should store their wheelchair in a climate-controlled area out of direct sunlight. They should schedule annual maintenance visits with their vendor.
Case Example: Tammy
Tammy had a stroke with dense hemiplegia. She was discharged home from a rehabilitation facility with a rental recliner. She could not tolerate sitting in her wheelchair because she fell to the left, leaving her bedbound. She was dependent for transfers via a mechanical lift, and her family was unable to transport her to appointments.
The home health social worker helped Tammy get a home visiting PCP.
Seating clinic for a tilt-in-space wheelchair with deep contour back and positioning cushion was completed in the home. The wheelchair allowed Tammy to get out of bed daily. This reduced the risk of aspiration, improved her cognition, and allowed her to enjoy visits with her family in her garden.
I am going to conclude with this case example. Tammy had a stroke with very dense hemiplegia. She was discharged from a rehabilitation facility with a rental recliner. Still, she could not tolerate sitting in a wheelchair because she constantly fell to the left, leaving her bedbound. She was dependent on transfers via a mechanical lift, and her family could not get her out to any appointments. We saw her in her home.
One of the biggest problems is that she did not have a PCP which made it difficult to get a provider to follow through with the seating and positioning process and get her a face-to-face evaluation. We involved social work, which brought in a visiting home PCP to assess her. Then, we saw her in a seating clinic and ordered her a tilt-in-space wheelchair with a deep, contoured back and a positioning cushion.
We evaluated her home to determine what might meet her needs. The vendor was able to mock up a seating system and bring in a few choices of backs and cushions. Ultimately, we could get her a tilt-in-space chair to allow her to get out of bed every day. This was great because she could take her meals in the chair, which reduced her risk of aspiration. It also improved her cognition and socialization with her family as she liked visiting with her family in her garden and getting outside to have additional stimulation.
Reevaluation
Falls
Pressure Injury
Pain
Functional Change
Medical Change
The seating and positioning process is not ever over. There are sure signs where a reevaluation may be indicated. The first one is falls. If the client has fallen in their seating system, we have to reevaluate why that is happening and if any modifications could make them safer. The second one is a pressure injury. We may need to collaborate with the vendor to create a pressure map to see how to improve their pressure distribution, pressure relief methods, or both. If they are having pain, not tolerating sitting, or changing function, these are also red flags. We see many clients who have degenerative diseases or declining function. We may need to modify their wheelchairs in these cases.
Ethical Considerations
I will conclude today by going through a few ethical considerations to think about as you engage in the seating and positioning process in the home.
Ethical Considerations: Access to Care
Home Health
Patient is homebound
Patient has needs that can be addressed in the home setting. Appropriate equipment available for demo.
Outpatient
Patient can travel to clinic.
Patient's needs cannot be addressed in the home setting. Patient requires complex equipment such as high-end electronics or complex positioning interventions.
The first consideration is always access to care. We are always deciding who we will see at home versus who we are going to send to an outpatient clinic for a formal seating clinic. If a patient is homebound, they can be best served in the home health setting. If the patient can travel to a clinic, I would consider sending them to an outpatient clinic.
I think the second thing is whether they have needs that can be addressed in the home health setting. Can I get the appropriate equipment for a demo? Can I get the people I need to do a proper postural assessment? Sometimes, a clients' needs cannot be addressed in the home health setting. I recently worked with a client who required complex high-end electronics and positioning interventions. The vendor and I felt that to develop the appropriate seating system, the client would be better served in a seating clinic. This client had a neurodegenerative disease and was going to be using alternative controls for driving. We had to develop a plan where the patient was discharged from home health to go to a seating clinic and then readmitted afterward. I developed a report of the client’s function to send to the clinic and I helped the client’s caregiver take some photos of his workstation to help the outpatient clinician understand his occupations at their visit. This process required us to do some complex problem-solving, but it was successful.
Ethical Considerations: Clinical Skill
Collaboration
Mentoring
Evidenced-based Practice
Continuing education courses
Manufacturer product catalogs
The second ethical consideration is clinician skill. How do I develop the skills that I need to be competent and confident in this area? The first area is collaboration. There is probably someone within your organization who has a diverse background in seating and positioning. Talking to them might be helpful. Perhaps, they can visit with your patient and provide you with input. Or, you may be able to work with a vendor or someone within the continuum of care (another therapist).
The second thing is mentoring. Can a therapist who has more experience in this area be a mentor to you and guide you through the process? You can always look at evidence-based practice to see what is out there. You could take a continuing education course such as you did today, and you can also look at manufacturers' product catalogs and websites. You can read blogs or look at your professional organization websites as these are all great resources.
Ethical Considerations: Choosing a Vendor
Relationships
Skill
Availability
The third ethical consideration is choosing a vendor. You have to make sure that the vendor is the most appropriate for your client and that you give the client a choice of who they would like to work with. Sometimes, you or the client have a pre-existing relationship and mutual trust with a vendor, but you need to be sure the vendor is the most appropriate to meet the clients’ needs and the client is on board in the selection process.
The second component is skill. Suppose you have a client that needs a specific intervention. In that case, there may be a vendor in your area who is good at working with clients who need alternative drive controls, molded seats, or work well with those with developmental disabilities. You might need to network with these particular vendors for these cases. Similarly, when you are talking to a vendor, you could ask, "Have you ever worked with a client like this before?" And, "What types of interventions have you used?"
The third thing I note when choosing a vendor is availability. Vendors may not be available to come out to a geographic location, or the timeslot is too far out. When this happened to me, I interviewed different vendors and found someone that could see them that week. An additional month waiting for an appointment is an extra month that that patient will not have the equipment they need.
Ethical Considerations: Access to Product Demonstrations
Client will be using equipment daily for several years so equipment selections must be carefully considered. Product demonstration is an essential part of this process.
Thorough assessment will guide product demonstration and narrow potential options.
Multiple visits may be required.
Transportation/space constraints.
Length of demonstration and loaner chair provision.
Another ethical consideration is access to product demonstrations. The client will be using the equipment that you choose daily for several years so equipment must be carefully considered. Product demonstration is an essential part of this process. You would not buy a car without test driving it. We cannot ask our clients to select a wheelchair without test driving it. A thorough assessment will guide the product demonstration and narrow the options. Sometimes, multiple visits are required. It is better to take more time to get the client what they need.
There may be transportation and space constraints. If your vendor is coming in a van, they might be making multiple appointments during the day and not have the ability to bring numerous bases. Or, they may have only space for so many backs. I have found that since COVID, some of the vendors have unloaded some of their demo stock because of concerns about infection control. Thus, it has been more challenging to get product demonstrations.
You also want to think about the length of the demonstration and if the vendor will provide a loaner chair, particularly if you have a client who does not have access to any appropriate mobility. I like to discuss this with the vendor before the seating clinic to see what the vendor is willing to do for the client until their final chair is delivered. This might make me choose one vendor over another. If the client is bedbound or cannot tolerate being out of bed without a loaner chair, I need to ensure that they have that during that time.
Ethical Considerations: Modifying an Existing Seating System
Access to Tools
Ability to Monitor Intervention Success
Benefit vs. Harm
Clinician Skill & Knowledge
Modifying an existing seating system may also be an ethical consideration. You may not have access to the appropriate tools or wrenches or the ability to monitor the intervention's success. I do not like to come in on a 30 or 45-minute visit and change something and not have the ability to go back and change it back if they do not like it. Adjusting legrests is an easy fix, and I can show the family how to revert to the original setting. Still, if it is something where I am loosening parts and pieces and not confident that they will be able to tolerate it, I do not like to do that.
Look at the benefit versus harm. Sometimes doing something is better than doing nothing, and sometimes doing nothing is better than doing something. If I am going to make a modification that can potentially impact the patient's skin integrity, I will be more cautious; whereas, modifying the length of the leg rest might require less monitoring time or something the caregivers can revert if needed.
The clinician needs to have the skill and knowledge to complete a wheelchair seating assessment. If individuals are not confident in their abilities, they need to talk it through with a vendor or a peer and ensure that they are following the correct protocol.
Ethical Considerations: Telehealth
In a sample of 48 veterans, a telehealth seating assessment (clinician on-site, vendor via telehealth) yielded high patient and provider satisfaction (Ott et al., 2020).
For a sufficient seating assessment, a skilled clinician must complete an in-person assessment.
The final ethical consideration is telehealth. With healthcare delivery modes changing, there has been a lot more telehealth. In a sample of 48 veterans, they found that they could do a telehealth seating assessment with the clinician on-site with the vendor via telehealth. With this model, they could yield high patient and provider satisfaction. I think the important part about this is that they could have a skilled clinician in person. Even though we are currently doing our seating evaluations primarily in person, I think telehealth will continue to grow. We need to be a little bit critical about how we use telehealth and seating and positioning.
Case Example: Agnes
Agnes had arthritis, diabetes, and obesity. She had slowly lost function and became confined to a recliner in her living room. She had several bouts of home care but did not make significant improvements in her mobility.
Her doctor put in a new referral for home care, and the physical therapist worked with Agnes to order a group 2 power chair. After initial training on the chair, she was able to accompany her husband to the grocery store, after not leaving her home for two years.
I will conclude with Agnes. She is my "feel-good" story. She had arthritis, diabetes, and obesity. She had pain and was slowly losing function. She became confined to a recliner in her living room. She had several bouts of home care, and they were focused on getting her to stand and walk, but she did not make significant improvements in her mobility. She had a new referral for home care. The physical therapist ordered her a Group II power chair. After initial training on the chair, she was able to accompany her husband to the grocery store, after not leaving her home for 2 years. She had freedom and mobility to go out of the house and access different parts of her home to pick out her clothing or whatever she needed to do. It was such a powerful intervention.
Home Health Best Practices
Identify seating champions within your agency
Build relationships with local vendors
Develop seating pathways to determine if a home-based seating clinic or referral to an outpatient seating clinic is most appropriate for your client
Home health best practice is identifying seating champions within your agency to be mentors and collaborators. It is also essential to build relationships with multiple vendors in your area to tap into their skills and knowledge. Lastly, it is vital to develop seating pathways to determine if a home-based eval or an outpatient seating clinic is appropriate for your client.
Summary
A wheelchair can make a profound impact on the user's well-being, independence, and comfort.
For those who are unable to travel to an outpatient seating clinic, home health offers the opportunity to procure a wheelchair.
The wheelchair consists of the base as well as seating and positioning components.
The therapist begins the process with a thorough assessment and works with a vendor to trial products to develop and order the most appropriate seating system for that client.
Training on the safe use of the wheelchair is an essential part of an effective seating intervention.
Questions and Answers
Are there any situations where Medicare will cover both a manual and power wheelchair within the same five years?
Medicare will not cover both. However, you may be able to justify this for a client who has a degenerative disease and has a manual wheelchair they can no longer use. This would be considered a change in status. You could document that they can no longer achieve adequate positioning or propel their manual wheelchair and that their existing equipment no longer meets their needs. You should be prepared to have those objective measures about why the existing equipment will not meet their needs.
Why do you have to discharge patients to a seating clinic and then readmit them to home health?
The only time when this happens is when they need to get to an outpatient seating clinic. Not every clinician has the same seating and positioning background, and the client cannot receive outpatient services and home services simultaneously. Based on this talk, I hope that you feel more prepared to do seating interventions in the home, but some cases are best served in an outpatient clinic.
Does a patient have to pay out of pocket if insurance does not cover DME?
Part of the funding process is that the vendor will run the insurance authorization and tell the patient their out-of-pocket expense. There are many different insurances and regulations, and these vary by policy and state. Where I have practiced, a client cannot be billed out of pocket for specific items if they have medical assistance; other things are not reimbursed. Examples might be seat elevation, a particular color, upgraded upholstery, or gold hand rims. If a patient wants something not covered by their insurance, I try to first talk to the vendor to find out the cost. If it is cost-prohibitive, sometimes the vendor can arrange the purchase a sample or demo equipment to save them some money.
What is the appropriate equipment for a client with a posterior pelvic tilt and sliding forward? What types of products are available?
I would first look at how flexible the pelvis is. I may place a towel to give them some lumbar support to see how that changes their posture? If they are sliding forward, I ensure they have appropriate permission under their femurs. They may also need a pelvic positioning belt to give them a postural cue. You can also add in seat slope, whether via an adjustable axle or adding a wedge in the front of their chair. Opening the back angle can also allow gravity to give them more support. Sometimes people slide themselves forward to feel more stable or comfortable. If this is the case, I may need to reevaluate their cushion. Finally, it may be because their hamstrings are tight and their legrests are elevated. The tight hamstrings pull the pelvis into a posterior tilt and promote sliding. In this case, I would lower the legrests and/or open the back angle.
References
Barbareschi, G., & Holloway, C. (2020). Understanding independent wheelchair transfers. Perspectives from stakeholders. Disability and rehabilitation. Assistive technology, 15(5), 545–552. https://doi.org/10.1080/17483107.2019.1594407
Best, K. L., Kirby, R. L., Smith, C., & MacLeod, D. A. (2005). Wheelchair skills training for community-based manual wheelchair users: a randomized controlled trial. Archives of physical medicine and rehabilitation, 86(12), 2316–2323. https://doi.org/10.1016/j.apmr.2005.07.300
Bigras, C., Owonuwa, D. D., Miller, W. C., & Archambault, P. S. (2020). A scoping review of powered wheelchair driving tasks and performance-based outcomes. Disability and rehabilitation. Assistive technology, 15(1), 76–91. https://doi.org/10.1080/17483107.2018.1527957
Citation
Frye, Sara (2022). Seating considerations in the home health setting. OccupationalTherapy.com, Article 5479. Available at www.occupationaltherapy.com
