Janet: Hi everyone. Thank you for taking this class. I hope that the title of this course sparked your interest and led you here today. To give you some background on me, I primarily practiced in the area of pediatrics as a SIPT (Sensory Integration and Praxis Tests) certified therapist, and owned two large sensory integration clinics. I have now expanded the sensory strategies that I have learned across the lifespan. My work with adults with autism, as well as other neurological and developmental challenges, has led me to be a consultant working with the adult population. Now I work in a large facility where we have pediatric inpatient, as well as, a skilled nursing unit and an outpatient center. I started to notice that dementia was on the rise, and that folks living with dementia could benefit from using sensory-based strategies. It is an area that is up and coming, and we are exploring it more. This course is an overview to offer some insights for occupational therapy practitioners to start to expand and offer our expertise in this area for these clients.
We will review quickly what I hope to accomplish in our course today. I want you to know how important engagement and functional activities are as occupational therapists. With this population, it is important to stay engaged to help these folks continue to live a very productive life. We also want to look at understanding and looking at the different levels of dementia. We often associate dementia with Alzheimer's disease, and they are actually two very different and distinct categories. We want to talk a little bit more about that so we have a basic level of understanding of dementia. Then, we want to talk about how our sensory systems change over time, and how this impacts folks living with dementia. We will also discuss some strategies that we can implement.
Dementia
Dementia Facts
Dementia affects individuals in all countries. This is not something that we see more in the U.S. Dementia is not a normal part of aging and worldwide statistics have changed. I looked at this statistic probably three months ago, and they have upped it from 35.6 million people, who were living with this disease back in 2012, and now the estimated number is 47 million people (WHO, May 2017). Roughly, there are 9.9 million new cases per year. In the year 2030, they expect that to rise by 75 million, and that number is expected to triple by the year 2050. I think that is staggering. Currently, only eight countries worldwide have national programs in place to address those living with this disease. Of these cases, 60% to 70% are Alzheimer's disease. However, that is not the only form of dementia. This is important to keep in mind as we progress forward with today's talk.
Dementia is not a specific disease. It is a descriptive term for a collection of symptoms that affect our brain. People who typically have dementia have impaired intellectual functioning that interferes with their normal activities and relationships. These individuals also lose their ability to solve problems and maintain emotional control. They also typically experience personality changes. You will see a lot of behavioral problems, such as agitation, hallucinations, and delusion. We see different behaviors such as pacing and hoarding, as this disease progresses. There are also a lot of other things that are related to some of the sensory challenges. While memory loss is a component of dementia, memory loss does not mean that the person has dementia. Doctors will only diagnose dementia if two or more brain functions, such as memory and language skills, are significantly impaired without having loss of consciousness. It cannot be related to a head injury.
When we look up the umbrella term of dementia, there are a 100 different conditions that impair memory, behaviors, and thinking, but the most common causes, and especially for those of us who are practicing in skilled nursing, rehab settings, or home care, are listed below.
- Alzheimer's dementia (AD)- 50-70% of cases
- Vascular dementia (VaD)- 20%
- Dementia with Lewy bodies (DLB)- 15%
- Parkinson's disease (PD)- 5%
- Fronto-temporal dementia (FTD)- 5%
There is a nice image that shows how dementia is an "umbrella" term on this website.
Vascular dementia.
This is the second most common form of dementia. This accounts for about 20% of all cases, and vascular dementia occurs when an individual has reduced blood supply to the brain. This is something that we usually see related to a secondary cause, typically a stroke.
Parkinson's disease.
I was actually was a little bit surprised by this statistic. This only accounts for 5% of the dementia cases. Parkinson's Disease is a degenerative disorder of our central nervous system. I feel that we might be seeing some of these numbers on the rise as well. We might not always be referred for Parkinson's disease patients. At my facility, for example, I think a lot of our folks are at home right now, and I am not seeing them in my skilled setting.
Fronto-temporal dementia.
Another 5% is related to the fronto-temporal dementia. This is caused by different proteins that have build up on the nerve cells.
Dementia with Lewy bodies.
I have seen this one quite a bit, and this accounts for 15% of all dementia cases.
Alzheimer's dementia.
This is caused by abnormal brain cells, and it accounts for 60% to 70% of all types of dementia that we see in skilled settings. When you start to work with this clients, it is important to know about staging and using a staging scale to determine their level of dementia.
Global Deterioration Scale
The Global Deterioration Scale is used to describe dementia, and this was the first scale initially developed to look at the stages of Alzheimer's disease in 1982 (see Figure 1).
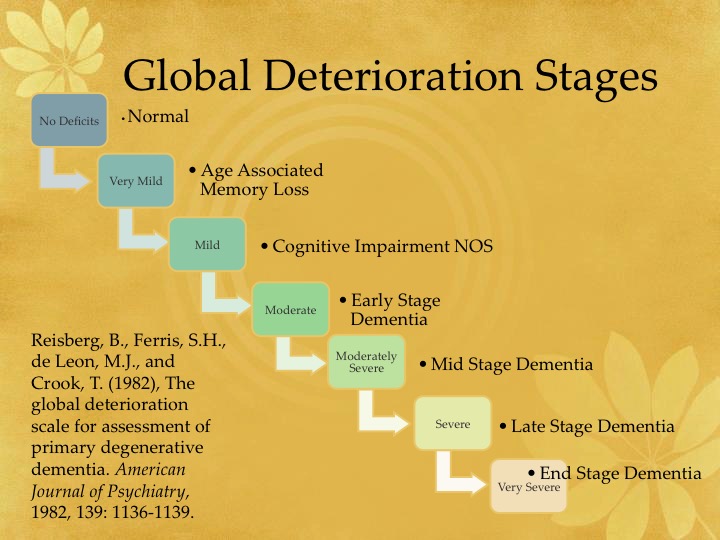
Figure 1. Global deterioration stages.
In the first three stages, we call these the pre-dementia stages, so we are not seeing a lot of significant decline in folks.
Stage one (pre-dementia).
Stage one is what they consider normal, or no cognitive decline. Typically at this stage of dementia, there are no significant problems.
Stage two (pre-dementia).
Stage two is referred to as very mild. This is where you might see occasional lapses of memory, forgetting placements of objects or names that were once familiar. I think we all kind of relate to this category at one time or another. This is a mild decline in memory. This is typically normal age-related cognitive decline, but it can be one of the early signs of degenerative dementia. You want to kind of keep an eye on that.
Stage three (mild or pre-dementia).
Stage three is also called the mild stage. This is where people might start to get lost easily, they might have poor performance at work, or consistently forget names of family members or close friends. There is also a lot of difficulty with concentration. Clients become aware of this, and that they may experience some mild to moderate anxiety with these symptoms. It starts to interfere with their day-to-day lives. The client and family are starting to notice things, but oftentimes they are still not going to see the physician and getting diagnosed at this early stage.
Stage four (moderate or early stage dementia).
This is also an early stage of dementia. This is when individuals might become socially withdrawn. They start to show some changes in their personality and moods. Often, there is a denial of the symptoms. Some of the behaviors to look for in this stage are decreased knowledge of current or recent events, difficulty remembering their personal history or background, and challenges with handling their every day activities like financing, making plans, organizing themselves, and coordinating their household. There is also a little bit of disorientation here. They start to have trouble recognizing familiar faces or traveling to familiar location. They will also start to avoid challenging situations, and try to hide symptoms to prevent stress or anxiety.
Stage five (moderately severe or mid stage dementia).
This is when they need some assistance to carry out activities in their daily lives. At this stage, they are unable to remember major details, such as their address and the names of close family members. It starts to interfere with basic functioning. They do not need assistance yet with physical activities, such as using the bathroom or eating, and they often still have the ability to remember their own names, their spouses, and their children, but we are starting to see some of the behaviors that we saw in the previous stages more consistently at this stage.
Stage six (severe or late stage dementia).
This is when folks start to forget the names of their children, spouses, or primary caregivers. They will need 24-hour kind care and often cannot be left alone. They also may display some delusional and obsessive behaviors, anxiety, aggression, and agitation. They may also wander. They have difficulty sleeping, and in some cases, they will start to experience some visual hallucinations.
Stage seven (very severe or end stage dementia).
This is referred to as very severe dementia or end stage dementia, along with the loss of motor skills. Patients progressively start to lose their ability to speak during this final stage. This is when the brain almost seems to lose its connection with the body. They need more physical assistance as well with tasks like eating and using the bathroom.
During all these stages, there are strategies that we can use to assist folks to make their lives more fulfilling and also to help take some of the stress off of the caregivers.
Strengths and Challenges
Now, as we know with every diagnosis, there are always strength and challenges (see Figure 2).
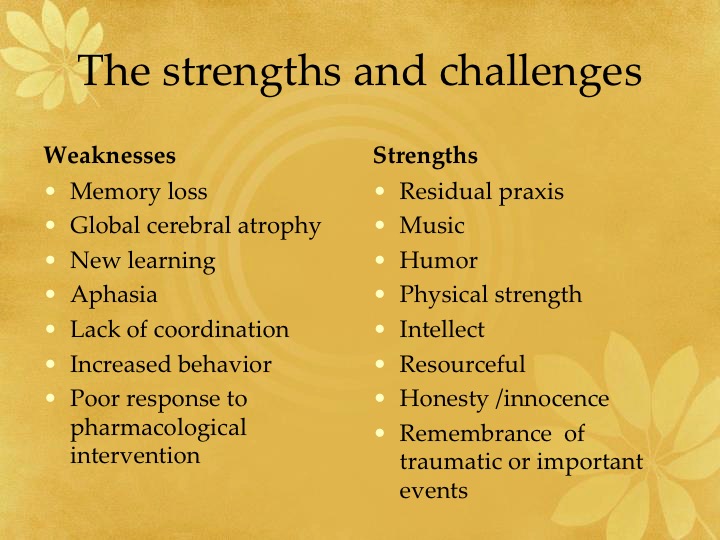
Figure 2. Strengths and challenges of people with dementia.
There are many challenges for folks that are living with dementia. Often, there are changes in memory, speech, and difficulty with new learning. There is a lack of coordination. We start to see some increased behaviors that were not typical for these individuals. We have also learned is that there is a poor response to pharmacological intervention. We will talk later about how pharmacological interventions are usually not effective with this population until some of the later stages. What research does show is that active engagement and being involved in activities can improve behaviors and limit challenging behaviors.
A lot of the strengths are still left. They can still perform activities that they have done over and over. For example, if somebody was a construction worker, they may still know how to put things together, use a hammer, or make simple crafts. We will talk a little bit later about activity kits. We have made several for the residents in my facility. One is a construction kit that has a hammer and golf tees, instead of nails. We have another gentleman loves our nuts and bolts activity kits. Music is such a powerful tool, and it is another area that stays very much intact. We know this across several different diagnoses, but there has been a lot of research to show the power of music, and how music can help you to bring a person back to a previous time and help to calm them down. We use music a lot. The other thing that I love when working with this population is that their sense of humor usually remains intact. We use a lot of humor to help them engage. They also are physically strong until nearer to the end stage. It is important to get them engaged in movement activities, and continue to walk and to do all those physical activities on a daily basis. Just because they have dementia does not mean that there is no intellect there. It is great when you get someone to talk about things in the past, or you have someone like an accountant who still has math skills. We see a lot of that. Never lose sight of that. These folks can be very resourceful. I think it is in our nature to try to go back into that survival mode. There can be real honesty, combined with a little bit of innocence. They will tell you how it is. I love that fact, and that can actually lend itself to a lot of humorous opportunities when working with them. The other thing that is good to remember is that these folks often remember important and traumatic events that have happened in their lives. This is important to note when bringing sensory strategies into an environment; especially the power of smell. Smell can evoke emotion, and you have to be careful that you are not triggering a traumatic memory. You might have to do some research before using sensory strategies.
Common Behaviors
There are some common behaviors that we start to see as dementia progresses (see Figure 3).
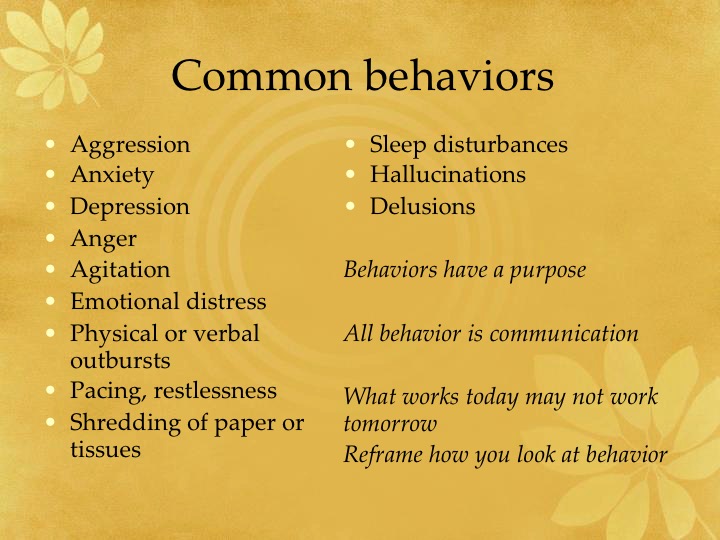
Figure 3. Common behaviors with dementia.
Often, you see anxiety and depression. There can also be anger, agitation, and aggression, but my experience has been that a lot of those behaviors are due to frustration. It could also be due to sensory overload in their environment that lends itself to emotional distress. Think about if you could not communicate to tell somebody that you did not like a smell, something was too loud, or that a person took something from you. We need to really be cognizant of that. Oftentimes, we will see a physical or a verbal outburst as a result. You start to see increased pacing and restlessness. For example, they may start to do things like shred paper or tissues. Sleep disturbances are common, as are hallucinations and delusions. They may demonstrate some hoarding behaviors. All behaviors have a purpose, and that all behavior is communication. When we are working with anybody that demonstrates challenging behaviors, you need to step back for a minute and put on a detective hat. We need to use our powers of observation to find out why this behavior is occurring. What was the environment like? What was going on? Put yourself in their shoes. How would you feel in that environment? I often ask myself, "Could you handle living here? What would you need to change about that environment?" I think this is true of any facility that we are working in. You need to reframe how you are looking at behavior, and remember it is all a sign of communication. When we are working with behavior issues, cookie cutter approaches do not work. What works one day, might not work the next day. You really have to take your time, put this strategy in place, and then go back and make sure it is working. I have seen therapist only give the resident one choice of something. It is the same for all of us. Some days you can handle a certain sensory input, and another day you cannot. This can even fluctuate hour to hour. For example, on your way into work, you might listen to loud, upbeat music. After a long stressful day at work, you turn on your car and you kind of jump because you cannot believe you listened to the radio at that volume. For the ride home, maybe you put on more of a classic radio station or something with more soothing input like talk radio.
