Kristi: Thank you so very much. That was a very kind introduction. I am going to ask you to grab a piece of paper and a pencil. There are times in this presentation that I am going to ask you to jot down ideas. This talk was originally given as a keynote at the Minnesota Occupational Therapy Association, having won a particular award called the Communication Award. Subsequently, a version of it is one of two distinguished speaker awards that I gave in Cleveland, so do note that this has been given before.
I want you to learn a little bit about your speaker (me). I think that is very important; as our narrative is very important. It shows you my narrative that brings me to where I am today. Each of you have your own narratives that have brought you to where you are today as a occupational therapy practitioner, as a faculty member, or as a student. Whatever walk of life you are in, you have a story that has brought you here today. My three mentors and dear friends are shown in this slide (Figure 1).

Figure 1. My mentors.
Rhoda Erhardt, who is up in the upper right, is an occupational therapist internationally known in pediatrics. I want to thank her. My friend, Dr. Judy Reisman, who is in the middle, is a professor at the University of Minnesota. She is a retired professor and was very involved in sensory integration therapy. Finally, Dr. Charles Christiansen, whom you see in the corner on the right. We did a duathlon. He is the former CEO of American Occupational Therapy Foundation and is a author of many books and articles that many of you probably have read. My family is in the left corner. I also want to give thanks to St. Catherine University, as they have supported me in giving talks all over the world. That does take time, and I really have a passion for listening to talks, hearing from other people, and learning.
Today, we are going to cover the personal perspective and how important that is to who we are as occupational therapists, or even who we are in any profession. I am going to give you a little bit about my story, and that story does lead me here today, as does your story. We are going to talk about how narrative is key to client-centered care and the therapeutic use of self, because if we do not stop and listen, and come to know our clients, we cannot effectively deliver our services. We are going to visit multiple ways of knowing and what that means, and how that contributes to evidence-based practice; that interface with the therapeutic use of self. Then, I am going to bring you through a few different conceptualizations of client-centered care and therapeutic use of self. We will talk about some theorists, some authors, and then also a relationship-based care program that I hope you get excited about as it can lead to improved quality of care at the systems level. Finally, we will apply it to the classroom and the fieldwork. The visual expressions throughout this PowerPoint are mostly mine. I have a affinity for taking a little point-and-shoot everywhere I go. Some are also from free sites or I have permission to use.
Dancing to the Beat of the Music
Why would I title this Dancing to the Beat of the Music? If you look in Figure 2, each of these photos depicts a different type of dance with a different culture, some individuals, some together, some are touching one another and some are parallel.

Figure 2. Dancing to the beat of the music.
Each type of dance has its own rhythm and beat, and yet, all of those types of dance are so important to the whole of the art of dance. Similarly, as occupational therapists, or anybody working in the healthcare field, we each have our own gifts that we bring to our therapy. Today, we are going to talk about some common elements that we might find in client-centered care or in therapeutic use of self, but we also have our own distinct interface with our clients, practitioners, students, or peers.
My Journey
Figure 3 depicts pictures of me growing up.
Figure 3. Family photos.
The bottom left is my family. I was born to a father who was an executive at a large company here in the Twin Cities, and a mother who was most likely to succeed; a homecoming queen, a concert pianist, and a concert vocalist. My brother was born two and a half years after me. Not too long after my father married my mother, she developed a very severe form of schizophrenia. It changed all of our lives. Miraculously, dad has stayed married to my mother, and they have been married 54 years, which is very rare for someone who has such significant schizophrenia. My childhood was met with adventure and fun, yet, my mom was in and out of the hospital. We had health practitioners working with us, and there was disarray at times. Beyond that, my mother had 16 shock treatments when she was pregnant with me. I was born blue, not breathing, with a collapsed lung and the umbilical cord around my neck, and nearly clinically dead. When I first saw my MRI, it made me cry; my brain looked worse than many of my clients. However, the brain is plastic, and we all have our own journey. It was this journey that probably led me to working in mental health as an occupational therapist and researching mental health and developmental disabilities. My little brother is also in the pictures. He and I were in a severe accident when he was four and I was seven, and it nearly killed him. He was left with learning disabilities and a brain injury, and he had epilepsy. Sadly, at age 30, in 1997, he had a epileptic seizure behind the wheel and had a single-car crash. Our family has dealt with health care on the side of being the recipients, in addition to my being on the side of being a provider. And through this journey, I have come to know that it is our relationship with whom we work that is so key. Early on, even as a kid, I could tell which healthcare practitioners cared about my mother or cared about my family and wished to partner with us in our journey. I could also identify the other health practitioners who were more likely to write everything off, or to be worried about the billing, or be worried about the next client. This is what gave me passion for therapeutic use of self in client-centered care.

Figure 4. Present day activities.
Fast-forward to present day, I am a professor and have been teaching aerobics and group fitness for 34 years. I am active in the Society for the Study of Occupation, which you see in the bottom right, some of my friends from there.

Figure 5. Present day activities continued.
As you can see, I am very active with athletics. The bottom right picture is my daughter and I doing a mud run. Why do I tell you all of this? It probably seems beyond something that is important for something on therapeutic use of self and client-centered care. But is not my story or your story so keenly important to what you bring to your profession and to your daily life? You know my story now, and I am hoping we each come to try to know the story of those we work with, the story of our colleagues, and the story of our friends, because it is then that we can truly understand the journey and how we can work with people and collaborate.
Evidence-Based Practice
Let's start by looking at this idea of evidence-based practice and how that might feed into the idea of therapeutic use of self and client-centered care. Since the 1980s, and extending to 1996 and Sackett's work on evidence-based medicine, including the use of research, clinical expertise, and patient values, healthcare professionals have often endorsed the hierarchical, two-dimensional graphic of evidence in Figure 6.
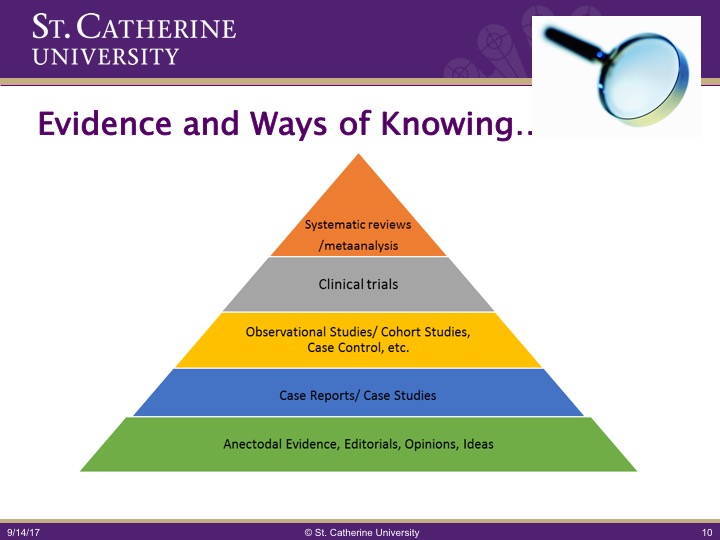
Figure 6. Levels of evidence.
At the top is a systematic review or a meta-analysis. Just below that are clinical trials, which often means double-blind trials, often in a clinic-controlled setting. While we know these are important, we must go beyond this. Countless articles, blogs, dialogues, and various scientific journals have challenged this original focus as too narrow. While I assert that evidence-based medicine in this hierarchy is important, we must go beyond this to think about other ways of knowing. In 2005, the then-president of the American Psychological Association (APA), Ronald Levant, developed the Presidential Evidence-Based Initiative, asserting that some evidence-based criteria was too narrow and that managed-care companies and malpractice lawyers could misuse the data. In response, the Evidence-Based Initiative sought to affirm the importance of multiple source of research and evidence, including multiple research designs and clinical expertise. I quote, "Each of these and how they play into your practice are important: ethnicity, race, culture, language, gender, sexual orientation, religion, age and disability status, and treatment acceptability and consumer choice." Let's think about that term consumer choice. How many of your clients have a choice to be with you? Some of them yes, some of them no. My practice has largely been working with persons with serious and persistent mental illness and/or serious developmental disabilities. Many of my clients are civilly committed in either the mental health forum under MI, mental illness, DD, developmental disabilities, or MI&D, mental illness and dangerous to the public. Most of these clients do not choose to be where they are, and thus, the ability to think beyond traditional evidence and come to know the client is very important.
Henry, Zaner, and Dittus, while acknowledging the importance of evidence-based medicine and healthcare, asserted that traditional conceptualizations of evidence-based medicine cannot accommodate concepts that, "resist quantitative analysis and therefore cannot logically differentiate between humans and machines." These authors say tacit knowing, or inherent knowing, is important such as when you know something but you cannot explain it. Similarly, while we may attempt, assure, and assess concepts of client-centered practice, there are certain constructs that are very difficult to study, and I would like you to think about these. How do these constructs play into your practice: faith, love, belief, and caring. These all transcend traditional means of measurement, and we do not usually conceptualize them as evidence, but are they not key to developing good relationship-based care? Thus, I assert while we practitioners must look at the evidence to guide our practice, we must also acknowledge dimensions such as human interaction and therapeutic use of self, and how integral that is to our practice.
Theory of Knowledge
Let's look at another concept, and this comes from the theory of knowledge groups. Theory of knowledge groups expand on ways of knowing as in Figure 7.
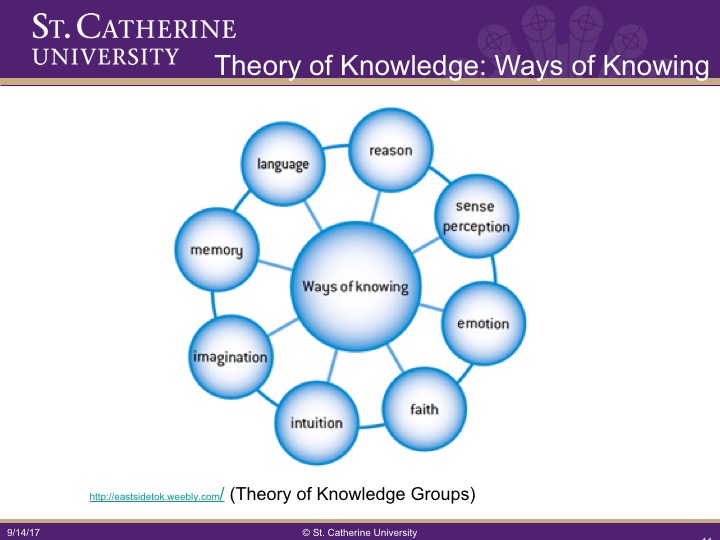
Figure 7. Theory of Knowledge.
I would like you to take a second and think about how these play into your own practice or your own everyday life. For instance, I am going to look at imagination. Imagination is something we may not originally think of as key to our practice, yet imagination is very important to practice, because we occupational therapists are constantly adapting. I am going to give you a clear example of one of my clients. This is one of my private-practice clients that I saw about six years ago. He is somebody who has both a psychiatric diagnosis and a severe developmental disability. He has fetal alcohol syndrome, autism, and is nonverbal. He was referred to me because he was spending 12 to 18 hours in a 24-hour period banging his head. The folks at the group home had lost hope and did not have any idea of what to do with him, nor was he having much in terms of productive occupation in his daily life. The first day I went and visited him, it was clear the group home staff cared about him but were at such a loss. They spent much of their time trying to protect his head in a plastic soft helmet to prevent further brain damage. They were trying to protect him, but at the same time, they were not offering him any opportunity for meaningful occupation. We looked at some sensory-based approaches for this, but it was not until I asked to see some of their puzzles and games, that we identified something to capture his attention. He was able to sit down with a large set of Legos for about 10 minutes and started constructing something meaningful. Yes, we used a sensory-based approach to calm him down to the point where he could do so, but it was then we realized that this man, originally thought to have a really low intelligence, was quite good at construction and in solving puzzles. From this, we were able to design an entire occupational plan for his day to maximize meaning and try to minimize that which was the overt focus, head banging.
Conceptualizing Therapeutic Use of Self
We are now going to take client-centered care and the multiple ways of knowing information and segue into a discussion of various schools of thought and theorists, and how they conceptualize therapeutic use of self. This is a picture of me with an individual that I worked with for many years and still see on occasion, but not professionally anymore.
Figure 8. Example of therapeutic use of self.
This is a photo from my book. This individual was written off by many because of her failure to talk very much or engage in conversation. It took time, listening, and observing. I bet you all can think about a client where rather than being so focused on getting the initial assessment done, you just spent 20 minutes observing, understanding, and coming to know what motivated that client. This is what I had to do with this client. This is so important, yet very difficult in this day and age with quotas, busy schedules, and more clients.
I am going to introduce you to See Me as a Person, and I am going to talk about it more later. See Me as a Person is a relationship-based care program near us in Minneapolis, St. Paul. It is from Creative Health Care Management and teaches healthcare systems relationship-based care. The authors, Mary Koloroutis and Michael Trout, are married. They are a nurse and a psychologist, and they authored a book called See Me as a Person and a curriculum. In this book, there is a beautiful poem written by Marge Piercy called the Tao of Touch. And as you listen to this, I would like you to think about how you use touch in your practice or in your daily life. That could be emotionally touching someone, or it could be physically touching someone.
