Learning Outcomes
- After this course, participants will be able to identify at least three critical skills to teach children with autism.
- After this course, participants will be able to describe the process for breaking down and teaching a new skill to a child with autism.
- After this course, participants will be able to list at least three strategies for teaching social skills to children with autism.
Introduction
Most of the work I do in the schools, at home, and in the clinic revolves around supporting students and children with autism. It is an area of practice that I feel passionate about. I work in schools supporting students with autism and other challenging behavior. I was looking at the polls and it looks like the majority of you are school-based providers. I feel your pain right now, as I know it is hard with everything that we are going through right now. We are in the same position ourselves with school-based services. It looks like many of you are outpatient providers, early intervention, and a little bit of mixed. It looks like the mix has varying degrees of experience working with children with autism. Common themes I found in the polling were challenging behaviors and creating sensory diets. In the first half of today's session, we are going to talk about critical skills, and then in the second part, we are going to get into social skills. All of these things together help with behavior and emotional regulation. I hope that I will get to most of your concerns. I love hearing from people so please reach out if I do not.
We are going to start by going over the characteristics of children with autism, that way we are familiar with what the diagnosis of autism is and what those characteristics look like in school, the home, and in the community. We are going to look at critical skills to teach those functional adaptive skills. I am going to go over strategies for teaching. Lastly, we are going to look at case studies and then have opportunities for questions and answers.
Resources: Padlet
- All resources available here:
- https://padlet.com/tara58/y70q8chmwq85m7cl
If you have not used Padlet, this is my new favorite thing. I am a technology guru, and Padlets are great tools that are free to use. I think you can create two of them for free, and then you can upgrade. It is a place where you can store a lot of information. You can add websites, PDFs, word documents, etc. This Padlet link has all the resources that I am going to go through in today's training, but now, it is all on one website for your convenience. If you go to that website, you can click and find any of the resources that I am going to share today. I have also used this to store information on other topics as well such as fine motor and social skills. I have used this in telehealth. It is a great resource for you to access as a therapist. And as a side note, any of these resources that I have included can be accessed as a PDF as well.
Autism Updates
- 1 in 54 children have a diagnosis of autism
- 4:1 boys to girls
- More children are being evaluated by three years old
- 84% of 4-year old children had received the first evaluation by the time they were three
- 1/3 to 1/2 notice a problem before the first birthday
- 80-90% before 24 months
(National Centers on Birth Defects and Developmental Disabilities, 2020).
Let's talk a little bit about the background and the current information on autism. Currently, 1 in 54 children has a diagnosis of autism. We see this more and more as children are getting diagnosed with autism. I also worry about how this is going to be impacted by COVID. I live in Oklahoma where it was hard getting access to evaluators before the pandemic. I wonder what we are going to see come out of this in six months to a year and if we are going to have more kids that are later diagnosed. Prior to COVID, most children were being evaluated by three years old.
Based on this information, 84% of four-year-old children received their first evaluation by the time they were three, a third to a half were noticed to have a problem before their first birthday, and 80% to 90% before 24 months. Many parents see these signs because we are doing more public awareness around autism as we are starting to become more aware of what to look for. Additionally, physicians are starting to be more aware and doing more screenings for autism. This is good practice as we know that the earlier we intervene, the better the prognosis.
It is hard to become an expert in everything that you do. These next couple of slides provide key points for you to think about as a provider.
What We Need to Know
- Signs by age of three - lifelong
- Combination of genes, biology, and environment
- Every day we learn more and more
- Comprehensive eval can diagnosis well before age of three
- Parents can learn new strategies and implement them within their routines
We can see those signs by the age of three. It is considered a lifelong disability as children do not outgrow autism. Children can definitely learn different skills and have very successful lives, but it does impact them throughout. It is a combination of genes, biology, and the environment. Every day we learn more about the diagnosis of autism. As mentioned earlier, a comprehensive eval can diagnose well before the age of three. Anybody who is good at testing can diagnose autism, or if they are seeing many of the early signs, children can be diagnosed before the age of three.
Parents can learn strategies to implement within their routines. A big piece of what we need to do is empower parents and teach them how to incorporate all these skills into their daily routines.
As Providers, We Need to Know
- What is autism?
- How did this happen?
- When did this happen?
- Why did this happen?
- What can we do about it?
- Where can we go for help?
As providers, it is important to consider these areas when you are starting to work with children with autism. For those of you who have worked with children with autism, I am sure you are in the same boat. I have been asked these questions many times, especially when working in early intervention. I know there are many of you that have an "elevator speech" or a response that you can provide when a parent asks you questions. You want a response that is objective and research-based and not something that you read on Google.
How did this happen? You want to reassure them that none of what mom did during pregnancy or their parenting skills caused this to happen. When did this happen? Why did this happen? What can we do about it? Where can we go for help? Think about how you are going to respond to those different questions.
What Families Want Us to Remember
- Give DIRECTION
- Know your stuff. We need information, resources, and ideas
- Give SUPPORT
- Think about the big picture
- Connect with other families who have children like theirs
- Give HOPE
- Help them feel in control again
- We know the road ahead will be filled with good times and bad
- Leaving you is hard
- Make sure we feel confident in our abilities to navigate that journey
These are good reminders about what families want us to remember. First, give direction. Know your stuff. Families who are telling us that they need information, resources, and ideas. Give them direction but do not overwhelm them.
Give support. Think about the big picture and connect them with other families who have children like theirs. Think about more than your therapy services and look at the bigger picture. They are going to learn so much from other families. And, oftentimes, it is much more than what we can provide them.
Give them hope. Help them feel in control again because all the families that I have talked to feel like they are out of control, and they do not know what to do. "We know the road ahead will be filled with good times and bad and leaving you is hard. Make sure we feel confident in our abilities to navigate that journey." It is always a hard transition from early intervention when they turn three whether they are going to school or outpatient. Help them to feel supported and that they are going to be alright.
This was a good reminder for me. As a provider, you can get caught up in what your goals are with that child instead of thinking about the bigger picture for that family and that child.
Possible "Red Flags"
- Not respond to name by 12 months
- Not pointing
- Lack of pretend play
- Avoiding eye contact
- Delayed speech
- Repeated words/phrases
- Upset by minor changes
- Obsessive interest
- Flap hands, rock body, spin
- Unusual reactions to sensory experiences
(CDC, 2020)
Red flags are things to look for in younger children. Not responding to their name by 12 months is one. Families often think it is their hearing. They get their hearing tested but they find that that is fine. If Dora the Explorer is playing, they can hear that, but they do not respond to their name. They are not pointing to communicate or to have those shared enjoyments. They have difficulty with pretend play. You might see kids who are lining up toys instead of playing with them. They might avoid eye contact and have delayed speech.
I worked with a set of twins where their speech was not delayed, but rather it was all over the place. They could not tell Mom what they wanted. For example, they wanted "juice," they spelled out planet names. You might see those repeated words or phrases over and over again with the same tone. They might be upset by minor changes. It could be something that most people view as a minor change, but the child has a hard time with it. They can have obsessive interests beyond, "I like playing with Thomas the Train." Thomas becomes all they can think about.
You might see hand flapping, rocking, and spinning. They might also have unusual reactions to sensory experiences. Often, you hear of children who have particular eating habits or only wear certain types of clothing.
Three Main Areas
Now, I am going to talk about three main areas: social skills, communication, and unusual interests and behaviors. These are characteristics of children with autism that we see across the community.
1)Social Skills
- Poor eye contact
- Prefers to play alone
- Does not share an interest with others
- Only interact to achieve the desired goal
- Flat or inappropriate facial expressions
- Difficulty with personal boundaries
- Avoids or resists physical contact
- Not comforted by others during distress
- Trouble understanding other people’s feelings or talking about their own feelings
(CDC, 2020)
For social skills, you may see poor eye contact. Poor eye contact is not a lack of eye contact. They may stare at you. It is not knowing how to use their eye contact in a socially appropriate way. They might prefer to play alone. It is not that they do not want to play with other people, it might be that they do not know how to play with people or have a fear of getting rejected. They often do not share interests with others. For instance, this is something that we look for on assessments. Do they share their enjoyment with somebody else? Did they hand the toy to their parent, or did they go over and show it to them? Their main purpose in interacting with you is to get a need met versus that social piece.
They may have difficulty with or display flat, inappropriate facial expressions. They do not know how to change their facial expressions based on the situation. I talked with an engineer at the university. He was talking about how he finally got a diagnosis of autism. I said, "Wow, how did that make you feel?" He said, "Well, it made me feel like I do exist on this planet." I said, "What are some things that you struggle the most with?" He said facial expression was a big thing for him. He said, "My girlfriend would tell me that my grandma died, and I did not know how to change my expressions to show her that I was sad." He said, "I did feel sad for her, but I did not know how to change my body and my facial expressions to show her that." They have many different feelings. I have heard from some families that they have more "feelings" than what we could even imagine. However, they do not know how to share that or how to read those cues from other people. I see many students with autism struggle knowing how to read the cues from their teachers. The teachers might say "sit down," and most of the other students can read if she is upset or if she is happy. The student with autism might have trouble with that.
They also have difficulty with personal boundaries. They might come up and give you a hug, but you have never met them before. Or, they avoid or resist physical contact and are not comforted by others during distress. They may have trouble understanding feelings or talking about their own feelings. Here is an example. I was texting back and forth with an 18-year-old. I said, "What are your three goals right now?" She has been doing well and she said, "I want to know how to better understand my feelings and how to tell people about my feelings." She often internalizes everything. This causes her to have a panic attack and stress out because she does not know how to talk about her feelings with other people. This can be challenging for many children with autism.
2)Communication
- Delayed or atypical language development
- Repeats words/phrases (echolalia)
- Reverses pronouns (you instead of I)
- Gives unrelated answers to questions
- Does not point or gesture
- Uses few gestures
- Flat, robot-like, or sing-song way
- Does not pretend in play
- Does not understand jokes, sarcasm, or teasing
(CDC, 2020)
Characteristics that you might see with communication are delayed or atypical language. You might see echolalia where they repeat the same way every single time. One of my favorite stories is I worked with a young girl who loved Dora the Explorer. Anytime she needed something, she would say "Backpack, backpack." The mom said, "Well, when Dora needs something she goes through her backpack." That was the way she told us what she needed. This is echolalic. It had a meaning to it, but it was repeated over and over. You might see some reverse pronouns like "you" instead of "I," which gives unrelated answers to questions. They also do not point or gesture. I talked about this earlier. They may also have a flat, robot, or "sing-songy" type of communication.
It can be hard for some kids to understand pretend play, understand jokes, sarcasm, or teasing. They have difficulty understanding the difference between teasing and bullying. I have a middle school and a high school student that give their friends and each other a hard time. For a child who has autism, that might be hard for them to understand that in certain situations people do that because they like you. It is not always a "bullying situation." Sometimes we tease each other because we like each other, and it is funny. It can be hard helping those children with autism to understand the intent behind a "bullying" situation and a situation where I am trying to interact with you in a "fun way." I completed a functional behavior assessment where a child was at recess, kids were joking around, and the child took it a whole different way. He fought the other kids, was sent to the office, and was kicked out of school. This can be a big deal for children with autism.
3)Unusual Interests and Behaviors
- Lines up boys or objects
- Plays with toys the same way
- Likes parts of objects
- Gets upset by minor changes
- Has obsessive interests
- Flaps hands, rocks body, or spins self
- Is very organized
- Circumscribed interests
- Rigid adherence to routines and rituals
(www.cdc.gov)
One of the first things that we notice is those unusual interests and outside "external" behaviors. They line up toys or objects, and they play with the toys the same way repeatedly. They may get caught up in the parts of the object versus the object as a whole. They may spin the wheel on the car instead of moving the car around. Obsessive interests take over, and that is all that they can think about. It may be one of those things where every conversation that they have comes back to that "obsessive interest," no matter what the conversation started off with.
Again, you might also see the flapping hands, rocking body, and spinning. While some with autism can be very organized, I have also had some who were very disorganized. They had a hard time knowing how to organize themselves and how to categorize certain things. They have circumscribed interests and rigid adherence to routines and rituals. As we as therapists tend to do, I had a boy that I tend to recall all the time. He had rigid adherence to rituals and routines. Here in Oklahoma, we have many trucks and cars that are Chevys and Fords. His parents lived in an apartment, and every morning they would walk through the parking lot to get to the bus. Every single time he went through that parking lot, he would do a certain motion to the Chevy cars or trucks and a certain motion to the Ford cars or trucks. He had this rigid adherence and they said, "If we do not do this, he is going to get upset." However, I feel the more we feed into it the worse it gets. We had to work on that by understanding what that behavior was about.
Other Symptoms
- Hyperactivity
- Impulsivity
- Short attention span
- Aggression
- Self-injury
- Unusual sleeping and eating habits
- Unusual mood or emotional reactions
- Lack of fear or more fear than expected
- Unusual reactions to sensory experiences
(CDC, 2020)
Other symptoms that you might see are hyperactivity, impulsivity, and a short attention span. There are many children with autism who also have attention deficit hyperactivity disorder. I also see aggression or self-injurious behavior, especially for those who have difficulty communicating what they need. We will talk more about that with our strategies. We need to understand the "why" behind the behavior and "what" they are trying to tell us.
I am sure you have seen unusual sleeping and eating habits. I have children who will stay up all night or will fall asleep and then get up at three in the morning and be awake all night. How can we intervene to help the parents to address these two symptoms?
You may also see unusual mood or emotional reactions with many ups and downs. I have had many children demonstrate a lack of fear or more fear than expected. For example, they may have no fear during safety situations. It is scary when you see children dart off into the streets. I have one close friend that lives by me and her son has no fear. He will find a way to get out of her house and go to the neighbor's pool. Luckily, he can swim, but it is scary nonetheless. Children who are hyper-focused or scared about something will show a lack of fear or more fear than expected which causes them much anxiety. As I said earlier, unusual reactions to certain sensory experiences can set them into panic mode.
The core diagnosis of autism is about social skills, communication, and rigid/repetitive behaviors. However, it is important to know that children will show these other symptoms as well. Also, if you are seeing these other symptoms, make sure not to ignore the core symptoms. Make sure to help families through it instead of saying, "Well, it is part of his autism." Sometimes we need to think about it separately. Yes, he or she does have a diagnosis of autism, but I am seeing that they are also very impulsive with hyperactivity. Do we also need to look at attention deficit hyperactivity disorder, mood disorder, or self-injurious behavior? What can we do? Anxiety is another big one. Make sure we are not overlooking that they might need help in all those areas as well.
Learn the Signs. Act Early.
The CDC has information on its website called "Learn the Signs. Act Early." They also have a lot of good screeners and developmental tools for tracking as in Figure 1.
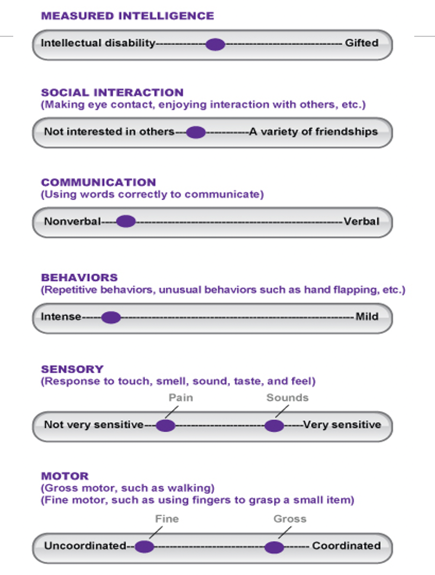
Figure 1. Example of the CDC's Free Milestone Tracker App.
I would highly recommend that you look at the Padlet that I provided and go through there to see what information you can share with families, teachers, and other providers.
Strengths
- Attention to detail
- Deep focus
- Observation skills
- Absorb and retain facts
- Visual skills
- Expertise
- Methodical approach
- Novel approaches
- Creativity
- Tenacity and resilience
- Accepting of differences
- Integrity
(Bennie, 2019)
I know I spent a good amount of time focusing on deficits. I would be remiss if I did not talk about strengths. I want to make sure we understand what is at the core of autism. One of my favorite quotes is, "If you have met one child with autism, you have met one child with autism." Each child is an individual, each family is different, and each child has their own set of strengths. And, each child and family have goals. How can we build on those strengths to help teach them those things that are hard for them?
One strength might be attention to detail. They may see details that we could never see, or it would take us a long time to see. I worked with a young man who I think is now 23 years old. For those of us who have been working a long time in this arena, it is amazing to follow these individuals from young ages to adulthood. I have not been seeing him the whole time, but I keep up with how he is doing. He has grown up fast. He has uncommon attention to detail. While he can communicate verbally, it is not a whole lot. I can get a puzzle out with many details, and he can put it together quicker faster than I ever could. It is amazing. They can also have deep focus. Being able to hyper-focus on one thing can be a skill. I seem to focus on 500 different things and cannot get anything done, but for some children with autism, this can be a really big strength. If they can focus on one area and learn that area well, they can do many things with that. I knew a guy that was interested in vacuums. He spent all his time looking at vacuums, researching vacuums, and he knew every make and model. Thank goodness there is somebody who does that because I need my vacuum to work. I do not want to learn about vacuums, but it can be an area of strength for somebody.
They may be able to observe and retain facts. Remember to use visuals as much as you can because many children have more visual strengths than they do auditory. They may have expertise in certain areas such as a methodical approach to doing things often in a novel or very systematic way.
Individuals with autism have creativity, tenacity, and resilience. They are much more accepting of differences. Often, there is such a nice innocence about many of the individuals I work regarding their integrity. They tell you how it is, give you their truth, and there is no intentional ill will behind it.
As you get to know your students and their families, you will figure out what their areas of strength are.
12 Guiding Principles
1. The earliest possible start to intervention is essential.
2. Services must be individualized for children and families
3. Family involvement and participation is critical
4. Families have a right to evidence-based services
(OCALI, 2020)
There are 12 guiding principles. These are a little bit more targeted towards early intervention, however, you can use these across the board. If you have not accessed the OCALI website, it is a good website. I think it is in my Padlet. There is a lot of good information on how to support children with autism, and it goes into specific interventions. It shows you the research behind it, and it gives you tools. It is a great website with all evidence-based principles for providing services to children with autism.
The first one is, as I mentioned before, is early intervention is essential. We need to make sure that we are looking for those cues and supporting families. If you are working a child with autism who is older, and they have siblings, you need to also keep an eye on them. Let families know some of those red flags to look for.
The second thing is that services must be individualized for children and families. I feel I am harping on this, but we have to look at individualized services. However, there are certain core things that we need to think about. When we are working on those critical skills, how can we individualize as much as possible?
Family involvement and participation is critical. Family support and involvement are the most evidence-based strategies out there. Remember, we are only with these children for a short amount of time. By involving families, we are giving them the hope and the support to do what we are asking them to do in therapy.
Families have a right to evidence-based services. We have to remember that we need to be using evidence-based practice.
5. Intervention is based on a developmental curriculum designed to address the specialized needs of the child with autism.
- Strengths and weaknesses
- Engagement, imitation, initiation, communication, playing reciprocal interactions, spontaneous interactions, making choices, following routines
(OCALI, 2020)
Intervention is based on a developmental curriculum designed to address the specialized needs with autism. Look at what their areas of strengths and weaknesses are including engagement, imitation, initiation, communication, reciprocal play, making choices, and following routines.
6. Intervention is planned and systematic
7. Regular and deliberate exposure to typically developing peers
8. Challenging behavior addressed through positive behavioral supports
9. Intervention should focus on developing communication skills
10. The development of social relationships is integral to successful outcomes.
11. Transitions should be well planned
We are using a curriculum that is targeted at the kids, but also as providers, we are supporting teachers with this. Intervention is planned and systematic. We are thinking about it ahead of time and teaching it in a systematic way. Regular and deliberate exposure to typically developing peers is another guiding principle. Are we supporting and making sure that children with autism are around their peers in a regular and deliberate way? This is not just as recess. We are making sure that we are being very deliberate about that. I am worried this next year about how it is going to look with people trying to limit exposure even more.
Challenging behavior is addressed through positive behavioral supports, and we are going to talk about that. What I am doing through this training is providing "positive behavior supports." Intervention should focus on communication skills by looking at how can we give children voices. Giving them a voice is one of the earliest things we can do. We can teach them self-advocacy and early communication. As occupational therapists, we need to make sure these children have a way to communicate. The development of social relationships is integral to successful outcomes. That is why we are going to talk about that today. Transitions should be well planned. When children are transitioned from early intervention to schools or from schools to graduation, this needs to be well-planned.
12. Getting to quality outcomes is not just about hours of direct services
- Intensity
- Fidelity of intervention delivery
- Social validity of goals
- Comprehensiveness of intervention
- Data based decision making (OCALI, 2020)
The last one is getting to quality outcomes is not about the hours of direct services. I know back in the day they had to get 40 hours of direct instruction every day or every week. Now, we need to make sure they are getting quality services. We are focusing on an intense skill, and that there is the fidelity of intervention where everybody is practicing the same way. There is social validity of goals, comprehension of intervention, and a database on decision making. We are making sure we look at all of these things and not at the clock trying to get to 40 hours.
Teaching New Skills: Where to Start?
- Motivation
- Motivation assessment
- Giving up a reward
- Functional communication
- Pointing
- Imitation
- Manding
- Adaptive skills
- Sitting
- Waiting
- Play/Leisure
Let's get started on these critical skills. This is, by far, my favorite thing to talk about. I love to teach new skills to children with autism or to children in general. For children with autism, it is even more important to be systematic in our approach, but these approaches can benefit many different children. The three areas that we are going to look at is motivation, functional communication, and adaptive skills.
Teaching Motivation (i.e. Reinforcement)
- The difference between positive reinforcement and bribery is all in the timing
- Positive reinforcement = continues the desired behavior
- Bribery = stops a challenging behavior
- It is critical to find what motivates the child and use to teach skills.
Motivation is usually one of the first places that I start. What is motivating to the child? If I can find what is motivating, I can teach about any skill. Motivation is also referred to sometimes as reinforcement. There is a difference between positive reinforcement and bribery. Most teachers and parents (including me) say, "Well, I do not feel like I should have to bribe a kid. The child should be doing it on their own." If you are saying or thinking that, you are misunderstanding what reinforcement is. Reinforcement is when I give something to a person or create a process where the behavior happens more often. Or, I do that to continue what I want them to do. Bribery stops the behavior if I give it to them. An example of this would be if I am taking my son to Walmart and he says, "Mom, I want that $80 Lego set." If I say no, but to stop the fit he is having on the floor, I do end up buying it, that is bribery. I gave him something to stop that behavior. They learn quickly what they need to do to get what they want. Positive reinforcement would be, "We are going to go to Walmart, and if you can help Mom get everything on the list, I will give you money towards a Lego set." That is the difference. I am going to reinforce him for doing what I want him to do. It is all about the timing. Try to embrace motivation and reinforcement as much as you can. It is been life-changing for me as an occupational therapist.
Finding Motivators
- Ask the family
- Observe the child’s play
- Reinforcer assessment
- Reinforcer checklist
- Experiment with new reinforcers
It is critical for us to find what motivates that child. I know many of us are getting started with the school year, find out what is motivating to them. Even if you are doing virtual service, find out what is motivating to them. Ask the family, observe the child's play, and look at what kinds of toys they are interested in.
Reinforcer Assessment
- List items in the item assessed box
- Select the first two items on the list, place them in front of the, observe which one they reach for
- Circle the item number the student reaches for and allow them to play with the toy for a minute
- Say “my turn” and remove the item
- Place the 1st and 3rd item and repeat
- Continue until all items as assessed
- Total the number of circled items for each number – highest is the most desired reward (http://www.schools.nyc.gov/)
There is a lot of different types of checklists out there. A reinforcer checklist is shown in Figure 2.
