Patricia: Hello to everyone. I am very glad to have you all coming in to talk about coaching today. We are going to be doing some activities that maybe you can even carry forward in the exact or similar format after this presentation. I began the coaching process because I recognized that over the years, I had been using a similar process with clients in the community, where we had to keep people functional and as independent as possible. The term coaching actually means different things to different people. Many of us think about the coach on the field or the athletic event, but coaching is really a strategy that has been used to change people's individual performance, and most importantly, to give them empowerment or skills that they can use for the rest of their lives. It is helping individuals to learn to solve their own problems and improve their own performance. The exciting part of coaching is that you are not the expert on the individuals life. They are the expert on their own life, and what we want to do is make sure that they will be able to use skills long after we have completed the process. Today, I am going to describe the coaching process and its benefits. Then, I am going to identify the evidence. The evidence is very solid outside occupational therapy and is rapidly increasing in occupational therapy. And then to give you some tools to walk away with today, we are going to talk about a few ways that you can begin the coaching process by using some tools.
Introduction
Now, I am going to ask you to take a piece of paper. I would like you to write down the words "continue, start, and stop." We always want to have people accountable for the outcomes of a learning experience or a session in which we have used coaching. One of the things I am going to ask you to do is as you go through the presentation, I want you to make it relevant to you, not relevant to anybody else. When you hear something that you are doing really well, salute yourself and say I need to continue to do this. On another vein, you may hear something that is totally new. When you do, write down a few notes to yourself. Sometimes we have bad habits that we want to stop doing. By the time we get to the end of the presentation, I am going to ask each one of you to write down what you are going to continue, start, or stop doing as a result of this presentation.
Expert Model
During a recent presentation in New Mexico on coaching, one of the therapists came up at the end of the presentation and said she was shocked. She said whenever she worked in pediatric home practice, she always asked the parents what they wanted the child to be able to do as a result of occupational therapy. However, when she went to skilled nursing facilities she did not do that. Instead she would say, "This is what we are going to be doing today." And she said, "You know, that is not too client-centered." She said that she was going to start asking the clients at the beginning of the session what their goals would be. Our goal is empowerment in coaching and developing self-efficacy for the jobs and the skills of living.
Therapist-centered Care:
- Directing therapy or teaching
- Providing solutions
- Identifying Cautioning
- Giving advice or suggestions
- Persuading or teaching
- Labeling
- Approving, or praising
- Analyzing Interpreting
The scenario above is what usually happens in health care. Our clients think that we are the experts. We are going to direct the therapy or teach somebody how to do something. We have the solutions. We are going to be identifying, cautioning, giving advice, and persuading. The terrible thing with labeling is that we have already decided what somebody is going to be able to do or not able to do. We also approve, praise, analyze and interpret. These are all therapist-centered activities.
Coaching Models
Coaching is moving out of that expert model.
- Therapist-centered care = teaching someone and helping them to learn
- Coaching = helping individual to improve performance; helping them to learn
You do not have to be an expert in something to try it. What you need to have is the motivation that it is important to you. What happens when we are not present with our clients? Are they dependent on us to be guiding the activities? Who really knows best what someone needs or wants, the context, or the personal expectation? We probably all have a story that we can talk about in our own therapy experiences. Fore example, when I worked in physical disabilities, I clearly knew my client needed to be able to shave. I set him up with an electric razor and got him to shave before his discharge. I was very proud of that. Then he announced to me as he was leaving that he did not have access to electricity. This is the kind of activity or event that we want to avoid. We want to give the skills for lifelong learning.
Positive Psychology
Some of you may have heard of positive psychology. Positive psychology is at the root of coaching. Positive psychology is a science that studies what makes life most worth living. It looks at positive human functioning. This is another big difference from the expert model, or what I will call the traditional therapy model. The traditional therapy model is that we know people have deficits, and we focus on getting those deficits to a more typical or normal pattern. In positive psychology, we look at adaptation and building on our clients' abilities. This is a positive psychology approach. They are going to be able to flourish based on their abilities, what they can develop, and improve, instead of focusing on the deficit model.
Some of you who have been around for while may have heard of Martin Seligman, who was the president of the American Psychological Association. He gave great value to positive psychology because it contributes the most to living a fulfilling life.
Flow Theory
You may have also heard of Csikszentmihalyi and his work on flow theory, which is also rooted in positive psychology.
Competence Cycle Model of Learning
We also have an investment in coaching in occupational therapy though the understanding that we teach confidence. We want to teach the skills for the job of living. You may have seen this Competency Cycle Model of Learning (Figure 1) before in the situational leadership research.
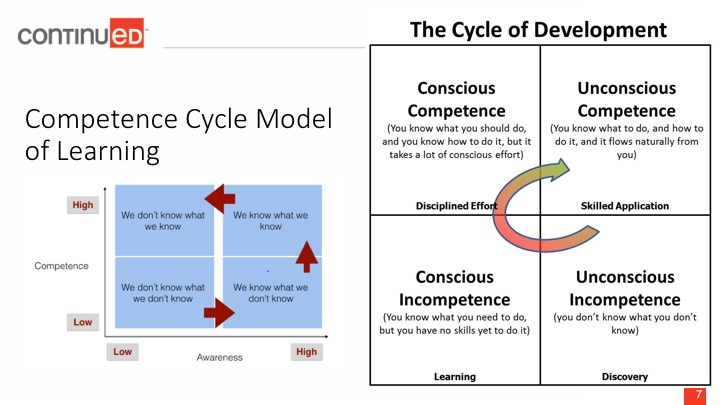
Figure 1. Competence Cycle Model of Learning.
This grid on the right shows moving a person from unconscious incompetence to unconscious competence. Situational leadership involves skills which are beyond what we are going to be talking today because we want to talk about specific goals of coaching. There are strategies that are used to move to these different levels.
Unconscious incompetence is you do not know what you do not know about something. This is probably one of the most dangerous situations to be in because you do not have an idea of what is even being expected. A good example would be presenting a new toy or activity to the individual which they have never seen before, and they do not know how to use it safely engage with it.
The second level is conscious incompetence. This is where you are aware of the lack of a particular skill. An example might be giving a client an hand crank can opener versus allowing them to use an electronic can opener.
Conscious competence is when you have learned how to do something, but you still need to think about it in order to do it. Another example of this would be asking a child to walk a balance beam, but they frequently fall off. Another is an adult trying to get better at buttoning their shirt one-handed. You all have watched this conscious competence cycle a lot in occupational therapy, because you can see the thinking and focused energy that needs to go into new skill acquisitions.
Then the last stage is the one where we truly have the person as their own expert, and that is unconscious competence. This is efficiency. If you drove a car this morning, you may have even driven through a light and did not even know whether it was red or green. Your body actually physically monitored that and knew whether you could proceed, and hopefully, you did it well because you are all on with me this morning. You no longer have to think about how to do it, but you just do it. In fact, if you think about it too hard, you may not be able to do it.
In contrast, if someone stops and asks me for my phone number, I have to pause for a moment, because I do not have to think about my phone number. Do I know it, absolutely. I know my mobile phone number, but I do not think about it on a daily basis. Another example is when they ask the last four digits of your social security number.
Coaching is this competence model in occupational therapy. We want to identify what stage the client is in. We want to use the language that is appropriate to move them to the next stage, and to try to get them to improve the skill that they are working on if they lack it.
Occupational Coaching
Occupational coaching is a term which I am going to use in this presentation. For those of you who know me a little bit better, I get a little frustrated that we always have to put "occupational" in front of the other word. Sometimes it isolates us from some of the major discussions around coaching. I am going to use it because I am seeing it a lot in the literature, and specifically about using this model in our practice.
What Is It?
We are trying to target improvement and performance, but the major goal is self-efficacy. People judge what they are able to do. If you judge that you can do something on your own, or do parts of an activity on your own, the literature shows you are more likely to do it. On the other hand, if you can the total ability to do something, but if you do not have self-efficacy, or the judgment that you are going to be able to do it, you will not try it. This has been demonstrated for years using Bandura's self-efficacy theory. We also see it play out in occupational coaching. We want to encourage experience so they develop that self-efficacy.
Coaching focuses on the here and now and getting ready for the future. It is not deficit-orientated, but rather it is competency-oriented. A good coach is going to believe that an individual has the answer to their own problems, and what we need to do is unlock them and then help them practice to develop that new self-efficacy (John Whitmore, in Coaching for Performance, 2009). If I had to summarize it at this point, I would say, you and I are not the expert. The individual working with you is the expert on their own life. This makes it patient-centered.
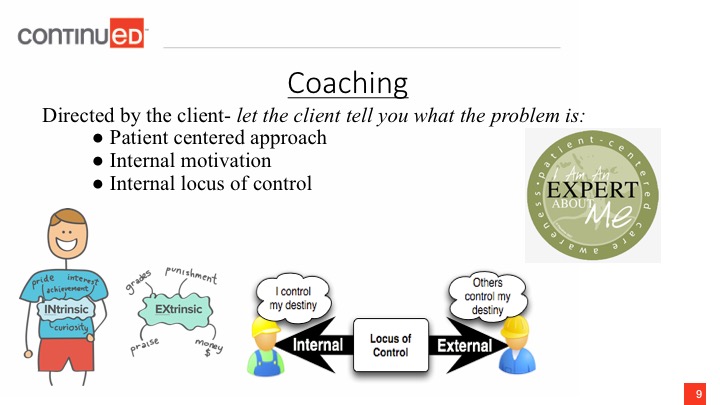
Figure 2. Coaching overview.
Again, we are working on that self-efficacy piece so we are going to be looking at moving from external motivation to internal motivation to practicing skills. We are moving toward an internal locus of control. This is much more empowering, and it drastically increases the self-efficacy.
What is Coaching?
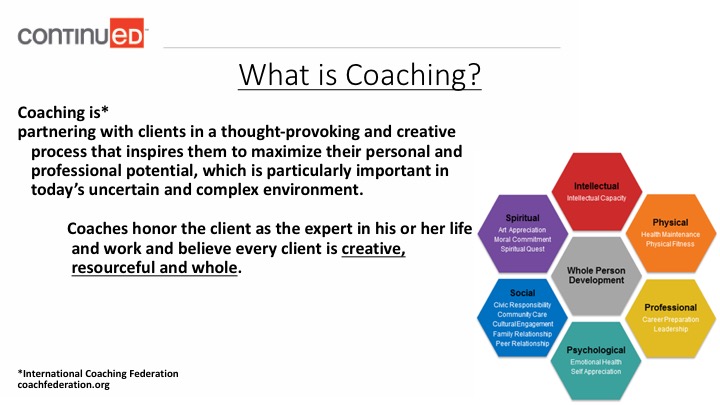
Figure 3. Whole person development constructs.
Coaching is partnering. I want you to underline that. You are a partner with clients in a thought provoking and creative process that inspires them to maximize their personal and professional potential. This is particularly important in today's uncertain or complex environment. Coaches honor the client as the expert in their own life because they believe that they have creativity, resourcefulness, and wholeness. Notice that the word wholeness is at the heart of coaching, which is a basic premise of occupational therapy as well. It is to be able to address and live life more fully with a greater quality of life, well-being, or whatever the individual is trying to pursue.
The diagram in Figure 3 is talking about whole person development. You can see the areas that are can be a developed in coaching and be taken on as characteristics of individuals which we need to address.
- Intellectual- intellectual capacity
- Physical- health maintenance, physical fitness
- Professional- career preparation, leadership
- Psychological- emotional health, self appreciation
- Social- civic responsibility, community care, cultural engagement, family relationships, peer relationships
- Spiritual- art appreciation, moral commitment, spiritual quest
The client during coaching is to initiate the goals and we are the facilitators. We are going to give them reassurance, and then we are also going to be also helping them reach that goal. The greatest challenge to us today, as OTs, is that we use checklists, protocols, and boundaries for our clients. Sometimes those get in the way of us actually understanding the goals of our clients.
I have talked with other therapists about being an underground therapist. It is clearly not important what we use to get to a goal. What is important is getting to the goal. The fastest way that we can do that is by using meaningful activity. My own children have laughed me using peanut butter and jelly sandwiches as a way to look at clients and help them along. But if that is an important food item to them and an important part of their independence, it does not matter what I use to get to the outcome. It matters that I do something that is meaningful and going to be inserted into the patient's life. This is at the heart of coaching also.
There are specific skills that need to be considered if you are going to be using coaching.
- Discover, clarify, and align with what the client wants to achieve
- Encourage client self-discovery
- Elicit client-generated solutions and strategies
- Hold the client responsible and accountable
First, you are going to use discovery. This is helping the client discover why, how, or what is preventing them from doing what they want to do. We also work with them on clarifying that so that they have a very specific goal. When I talk about alignment in coaching, I am talking about aligning yourself with the clients goals for achievement.
