Laura: I want to thank everyone for being part of this today because I think this is a very important topic and something that is considered an emerging practice area. The evidence available in the world of pediatric oncology has some catching up to do with the adult world of rehab oncology, but we are making progress.
Overview, Diagnosis, Incidence and Survival Rates
What is Cancer?
According to the National Cancer Institute in 2017,
"Cancer is the name given "to a collection of related diseases. In all types of cancer, some of the body's cells begin to divide without stopping and spread to surrounding tissues."
Statistics
There are hundreds of different types of pediatric cancer. The range in pediatrics is just as big as the range of adult cancer. It is the leading cause of death by disease in infants through 14 years, the second leading cause of death in children (second to accidents and trauma), and there will be an estimated new 10,270 new cases of pediatric cancer (ages 0-14 years) in the US alone (American Cancer Society, 2017). It is an important area of practice to be aware of.
Diagnosis and Staging
In terms of diagnosis and staging, there are different scans used.
- Fine needle aspiration (FNA)
- Ultrasound or CT scan
- Biopsy (needle, incision, or excision)
- MRI
- PET
- BMA
Fine needle aspiration is a superficial biopsy. If there is a mass or tumor under the level of the skin, they would do a fine needle aspiration. Ultrasounds and CT scans are often used to identify the location and size of the tumor. There are different types of biopsy, just a simple needle biopsy or incision or excision, and that is related to how invasive the biopsy is. MRIs, PET scans, and bone marrow aspirates are also used to confirm the diagnosis of cancer.
The TNM staging scale is related to diagnosing the stage of cancer. T is for tumor, and that is related to the extent, or the size and location. Regional lymph nodes is what the N represents. Has it spread to the lymph nodes and how many? There is usually a number associated with this. And then M is related to the metastases. Has the tumor metastasized to other areas of the body?
Common Cancers Among Children
Figure 1 represents common cancers among children.
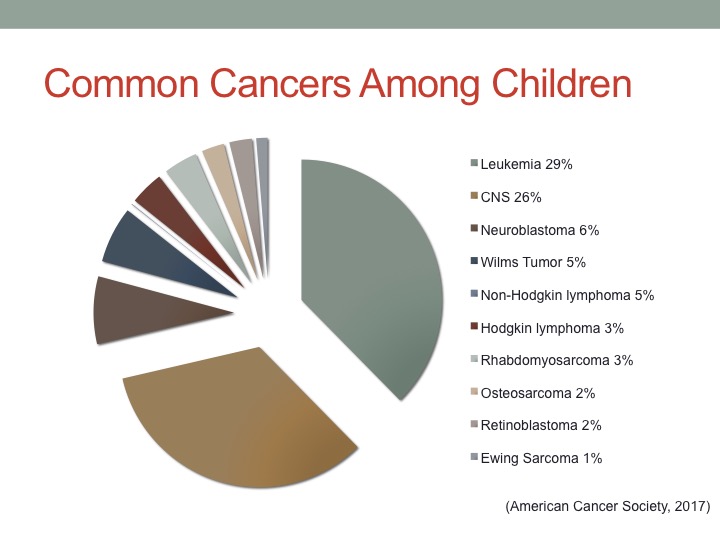
Figure 1. Common cancers in children.
Leukemia is the most common type of childhood cancer, making up 29%. This is related to blood cancers. There are many different types of leukemia, and we will go into more detail in just a few minutes. Central nervous system tumors are brain or spinal tumors and make up about 26% of the cases. Neuroblastomas are the third most common, making up 6%. This is a cancer of the nervous system, so along nerve fibers. Wilms tumor or kidney tumors make up 5%, followed by lymphoma, which is cancer involving lymph nodes and the lymphatic system. Rhabdomyosarcoma, which is very rare, is about 3%. This is cancer of soft tissue, and this may be found in muscle fibers and really all throughout the body. Osteosarcoma is a type of bone cancer found in adolescents, making up 2%. Retinoblastoma is cancer of the eye, and this is rare, making up for 2%. Finally Ewing sarcoma is another type of bone cancer found in adolescents, making up 1%. Throughout the remainder of this course, we are going to highlight some important things I think you should know about leukemia, CNS cancers, and neuroblastoma because they are the most common. These will be our primary focus today.
Pediatric Survival Rates
Survival rates are on the rise (American Cancer Society, 2017). As I mentioned there are many types of pediatric cancer and on average the current five-year survival rate is 83% (58% in 1970). That continues to increase. This is really exciting. There is a new emphasis on quality of life for these patients and that is where OT can come in. It is important to appreciate this even if you do not work in a cancer specialty institution as you might work with a pediatric cancer survivor. So understanding the impact of their treatment and disease process is important.
Pediatric Cancer Treatment and Functional Implications
Pediatric Cancer Treatment
Pediatric cancer treatment usually involves these things:
- Chemotherapy
- Radiation Therapy
- Stem Cell Transplant
- Surgery
- Steroids
- Immunotherapy
Chemotherapy is medication administered to treat cancer. The goal of chemo may be to prevent cancer cell growth, to slow cancer cell growth, to stop cancer cell growth, or it may be palliative to help someone become more comfortable. It depends on where they are in the continuum of care. This will also determine the type of chemotherapy administered. Radiation therapy is a more localized therapy that is administered usually with an internal beam or external radiation beam. Again, it is used to treat a localized area of disease. Stem cell transplants are intended to replace unhealthy bone marrow. They are used for a wide variety of malignant and nonmalignant conditions, but are are used to replace unhealthy bone marrow. Surgery is often used to remove solid tumors.
There are other types of surgery that these individuals undergo during treatment, for example line placements, or mediport placements, g-tube placements, etc. Steroids and immunotherapy can be effective to boost someone's immune system. Those are also different treatment modalities used throughout pediatric cancer treatment. Figure 2 is an example of a mediport.
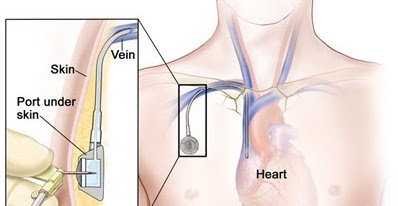
Figure 2. Mediport.
It is a line placed where chemotherapy can be administered and blood can be drawn. Usually these things happen every day for individuals in the active treatment phase. Thus, ports are placed so they do not have to have multiple needle sticks every day. They are usually placed for long-term treatment.
In the maintenance phase, when kids are ready to transition back to school and playing sports, a milestone in their care and in the hospital setting at Memorial Sloan Kettering was to come see the OT in the outpatient clinic to make a chest plate. We would fabricate chest plates to shield the mediport's location before they were removed to prepare them to transition back to sports, like soccer and baseball. That was an exciting milestone to be part of in the OT department.
General Side Effects
We could talk about these all day. These definitely impact occupational performance (Steomberg. Asher, Bailey & Fu, 2015).
- Mucositis
- Cardiopulmonary
- Fatigue
- Pain
Mucositis involves sores throughout the digestive system, primarily in the mouth. It can be very painful, making swallowing and eating difficult. Of course, this also impacts nutrition, which maintaining a nutritious diet is important in the healing process. If they are not eating enough, that may contribute to fatigue and not having enough energy to participate in some of the activities they are interested in. Some types of chemotherapy have cardiovascular implications and side effects. Endurance is usually an issue, and fatigue can be a result of cancer, or chemotherapy and radiation. Those can certainly impair function. Fatigue and generalized pain can also be an issue.
Neurological Dysfunction
Different types of neurological dysfunction may also develop as a result of chemotherapy or radiation (Lee, Arrillaga-Romany, & Wen, 2012; Stubblefield & O’Dell, 2009).
- Chemotherapy-induced peripheral neuropathy (CIPN)
- Radiation fibrosis
- Radiculopathy
- Steroid myopathy
Chemotherapy-induced peripheral neuropathy is common after certain neurotoxic chemos are administered. We will get into more details regarding CIPN in just a few minutes. Radiation fibrosis occurs when damage is done to healthy cells in the radiation field. That is one of the negative things about radiation. Many times, in the margins of the localized area that they are trying to treat, the healthy tissues are affected. Radiculopathy or radiating pain, can occur as well as steroid myopathy. Steroid myopathy usually presents as proximal muscular weakness, which may certainly impact function in severe cases.
Decreased Functional Performance
Many body structures and functions under the OT Practice Framework are impacted by the side effects of cancer treatment alone (Ness et al., 2009; Steinberg, Asher, Bailey & Fu, 2015).
- Decreased ADLs and decreased cognition
- Decreased strength, flexibility, endurance, balance and decreased peer interaction, motivation, self-esteem, poor social outcomes
This does not include the side effects of the actual disease process. I hope you can appreciate the impact it could potentially have functionally and psychosocially for a pediatric population.
