Editor's note: This text-based course is a transcript of the webinar, Stroke Rehabilitation: Vagus Nerve Stimulation And Virtual And Augmented Reality, presented by Tina Dimopoulos, OTD, OTR/L, CHT, STOTT PILATES® Certified Instructor for Mat and Reformer.
*Please also use the handout with this text course to supplement the material.
Learning Outcomes
- After this course, participants will be able to describe the therapeutic principles of vagus nerve stimulation (VNS) and virtual and augmented reality (VR/AR) as evidence-based interventions in stroke rehabilitation.
- After this course, participants will be able to explain how vagus nerve stimulation (VNS) and virtual and augmented reality (VR/AR) support neuroplasticity and motor recovery within occupation-based therapeutic frameworks.
- After this course, participants will be able to identify key clinical considerations for integrating vagus nerve stimulation (VNS) and virtual and augmented reality (VR/AR) into client-centered occupational therapy treatment.
Introduction
I am very excited to be back with OccupationalTherapy.com for today's presentation.
As an occupational therapy practitioner (OTP), I find it essential to stay at the forefront of neurological recovery in our clinical practice. My goal is to guide you through the emerging evidence and practical applications of these technologies. We will explore how vagus nerve stimulation can be integrated into traditional motor learning tasks and how virtual and augmented reality environments can provide the high repetition and engagement necessary for cortical reorganization. I have seen firsthand how these tools can shift the needle for patients who have plateaued in traditional therapy, and I look forward to sharing those insights with you today.
Emerging Areas in Stroke Rehabilitation
When I think about stroke rehabilitation and emerging areas, I often see vagus nerve stimulation (VNS) and virtual or augmented reality referred to as VR/AR among the most prominent areas of focus in our field. The integration of these services represents a truly innovative shift in practice. It is essential for us to understand how these technologies can be used to complement our traditional therapy approaches rather than replace them. By incorporating these tools, we can provide care that remains deeply client-centered and occupation-based while significantly enhancing motor recovery and neuroplasticity. This synergy is what ultimately allows our clients to achieve the most optimal functional return possible.
Vagus Nerve Stimulation (VNS) & Stroke Rehabilitation
I will begin today's lecture by discussing vagus nerve stimulation and stroke rehabilitation. Before we get too far into what vagus nerve stimulation is, let us start with a brief reminder of the vagus nerve function.
Vagus Nerve Function
The vagus nerve plays a critical role within the autonomic nervous system, specifically the parasympathetic branch, and helps maintain the body's homeostasis. I find it helpful to remember its diverse roles in heart rate and blood pressure regulation, respiratory rate, and mood and stress regulation through its connections to the limbic system. Reducing inflammation is another of its key roles, as is stimulating digestive enzymes.
Additionally, there are significant roles with oral motor and speech functions. Lastly, an important point for us to note is the research and growing understanding of the vagus nerve's role in promoting neuroplasticity, which is one of the primary reasons I am discussing it with you today.
Types of Vagus Nerve Stimulation (VNS)
When talking about vagus nerve stimulation, there are two different types of options: invasive and noninvasive vagus nerve stimulation.
Invasive VNS
Invasive vagus nerve stimulation involves electrical signals sent through a pulse generator implanted in the chest, which connects to the client's left vagus nerve. It is important to note that the vagus nerve stimulation is intentionally placed on the left side of the client's body to target that nerve. This choice reduces the risk of any cardiac or cardiovascular concerns. There is a higher risk of affecting heart rate and cardiac rhythm if the right vagus nerve is stimulated instead. I always like to point out to my colleagues that selecting the left vagus nerve is intentional for these safety reasons.
Non-Invasive VNS
Noninvasive vagus nerve stimulation does not require any type of surgical implantation. It involves an electrode that is placed by the ear or neck and stimulates the vagus nerve through placement on the skin.
VNS: Paired Vagus Nerve Stimulation (VNS) for Rehabilitation
Diving deeper into vagus nerve stimulation, I want to discuss the actual stimulation process known as paired vagus nerve stimulation. This phrase is often used with this approach, and the pairing occurs when the nerve is primed. The timing of the electrical stimulation is coordinated with a specific motor task. Vagus nerve stimulation is used during an activity, specifically during a functional task such as reaching. It is activity-dependent stimulation that requires me as the occupational therapy practitioner to monitor when the client is moving to pair the stimulation of the left vagus nerve. At the peak of the functional task, for example, when reaching towards an object or grasping a cup of water or manipulating a set of keys, I can then activate the vagus nerve trigger. This is typically done from a laptop interface, which connects to a wireless transmitter that sends impulses to the pulse generator.
I have a nice image that I will share in a few slides to help you visualize what I am describing here. As you can see, vagus nerve stimulation for rehabilitation should be activity-dependent. I am present as the clinician to help trigger or pair that stimulation intentionally. That stimulation should occur within milliseconds of the movement of touching or reaching for that functional item to really reinforce the specific neural circuit being used.
VNS: Neurological Mechanism
Diving a little deeper into the neurological mechanism, the vagus nerve interface consists of a lead wire with a cuff electrode that delivers a mild electrical pulse to the left vagus nerve. When neurotransmitter release occurs, it actually stimulates signals to the brainstem, which then travel to the motor cortex. When these chemicals are released, they create a window of plasticity that makes the brain more receptive to cortical mapping.
In Figure 1, you can see that the generator is located in the upper quadrant of the client, with a lead extending towards the electrodes on the left vagus nerve.
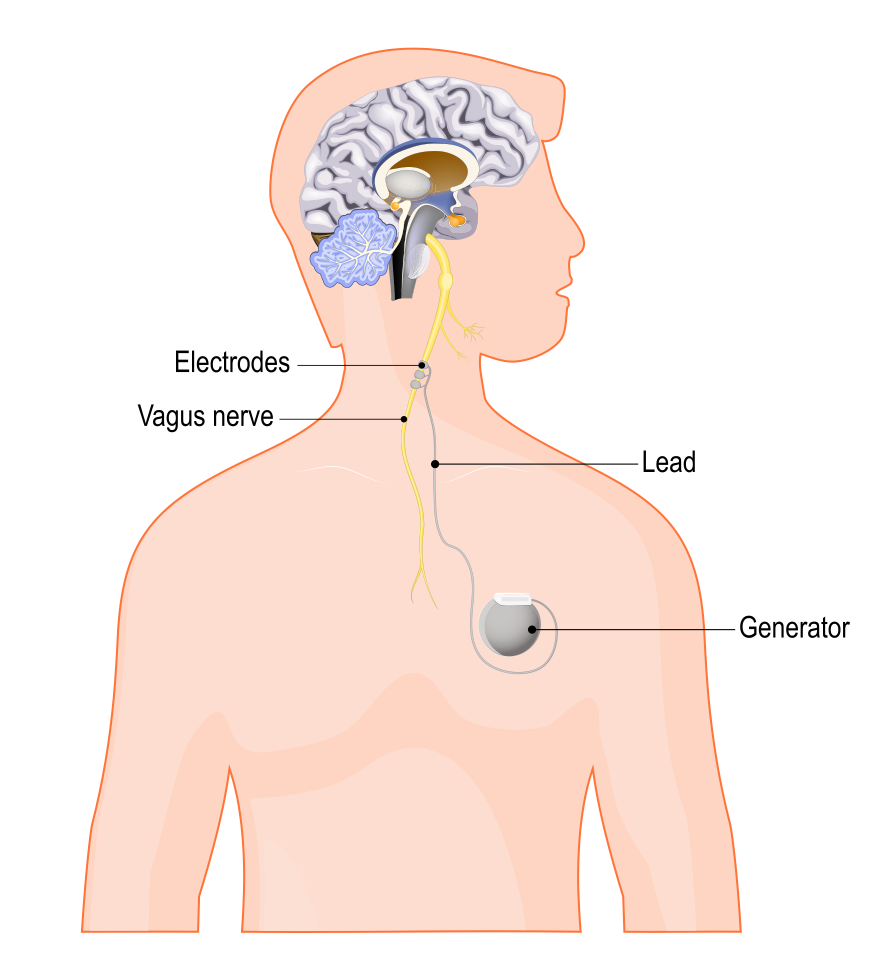
Figure 1. Vagus nerve stimulation device.
That vagus nerve then continues up towards the brainstem and the brain. This gives a nice visual to the prior slides and my description of vagus nerve stimulation. Here, you are seeing that the generator is implanted, so this would be the invasive approach.
VNS Supporting Research
What is the research saying about vagus nerve stimulation? It is important to note that the research supports vagus nerve stimulation as an adjunct to traditional therapy approaches. I will mention this throughout today's presentation because research indicates significant improvements in upper extremity motor function, motor control, and neuroplasticity. This occurs when vagus nerve stimulation is used as an adjunct to traditional therapy. The majority of the research with vagus nerve stimulation is currently focused more on ischemic stroke, and that is something that is important to note.
The reason we see more focus on ischemic stroke and less on hemorrhage is that, with ischemic stroke, neural networks are better preserved and therefore have a higher chance of being strengthened through activity-dependent neuroplasticity. Simply said, the neurons are injured but not dead, and therefore, more of the benefit of vagus nerve stimulation from a research perspective has supported ischemic stroke findings.
Additionally, there is an overall improvement in Fugl Meyer scores for participants with upper extremity function. Participants who have gone through vagus nerve stimulation with traditional therapy approaches show greater gains compared to those who did not have any vagus nerve stimulation used as an adjunct. Some studies have found retention of motor control and neuroplasticity up to three years post vagus nerve stimulation. An important component to highlight is that vagus nerve stimulation, when used in a rehab perspective, is and should be goal-directed, activity-dependent, and include purposeful movements of the client. It is important to remember that these are key elements for gaining more neuroplasticity and motor control through action-dependent, functional, and purposeful movements. Supporting research also emphasizes this.
Study Protocol for a Pivotal Randomized Study Assessing Vagus Nerve Stimulation During Rehabilitation for Improved Upper Limb Motor Function After Stroke (Kimberley et al., 2019)
This is a randomized, double-blind pilot study assessing vagus nerve stimulation during upper-limb rehabilitation after stroke. Clients looked at in this study were nine months to ten years post stroke, so we are looking at a more chronic onset here. Again, therapy was focused on functional and repetitive use of the upper extremity. Researchers found improvements in the Fugl Meyer and in the clinician's role. It really highlighted that, as the clinician is present during vagus nerve stimulation, the clinician can modify tasks and adjust upgrades or downgrades based on how the client is presenting. Additionally, each task was practiced at least thirty times every session. This study provided specific information on the type of repetition and the clinician's key clinical role.
I also want to dive into this chart here, which highlights how the vagus nerve is stimulated.
VNS Triggering Task Categories
Task Category | Example Actions | VNS Triggering Events |
Reach and grasp objects | a. Reach and grasp a cup
b. Place cup on different part of table/shelf | 1. When hand contacts cup |
Gross movement | a. Reach a hat on a high shelf
b. Place hat on top of head
c. Move hat to back pocket
d. Return hat to the shelf | 1. When hand contacts hat
2. When hat touches head
3. When hat touches back pocket
4. When hat is released on shelf |
Flip objects | a. Reach and grasp envelope on tabletop
b. Flip envelope over to the other side
c. Place envelope back on tabletop | 1. When envelope is grasped |
Eating tasks | a. Grasp a spoon placed in a bowl
b. Scoop simulated food with spoon
c. Attempt to pick up food | 1. When hand contacts spoon
2. When subject attempts to pick food
3. When spoon is lifted |
Insert objects | a. Grasp a die
b. Insert die into a jar | 1. When die enters the opening of jar |
Open and close containers | a. Open: Grasp jar with less affected hand; twist lid with more affected hand.
b. Close: Grasp lid with more affected hand; close jar and return to table. | 1. When hand contacts lid to open jar
2. When lid contacts jar to close it |
Patient-specific goal | a. Handwriting, self-care, playing an instrument | Varies with task |
For example, in the first column and first row of this chart, you will see that the example of a reaching and grasping task is the client reaching with their affected limb towards a cup. The clinician will stimulate or trigger the vagus nerve when the hand contacts the cup, specifically the pairing mentioned before. Ideally, the clinician can stimulate that nerve within milliseconds of the hand contacting the cup and can adjust or downgrade as needed to maximize the client's opportunity for the client to have motor recovery and relearning. When looking at a gross motor example, such as reaching for a hat on a higher shelf, the client will reach for the hat, and the therapist will trigger the vagus nerve via that laptop interface when the client's hand contacts the hat.
Moving a few rows down to an eating task and activity, the vagus nerve would be triggered by the therapist when the client grasps the spoon placed in the bowl. If the client is taking the spoon to the mouth, the vagus nerve could then be stimulated when the spoon has left the bowl and is directed to the mouth. I thought this chart was very nice because it gives not only functional examples for a task category, but also specific examples of when the clinician would want to trigger the vagus nerve. Triggering should occur within milliseconds through that laptop interface. In my opinion, this really demonstrates the key role of the occupational therapist in using this emerging, innovative technology in a rehab setting.
Vagus Nerve Stimulation Paired With Upper-Limb Rehabilitation After Stroke: 2- and 3-Year Follow-up From the Pilot Study (Francisco et al., 2023)
Continuing with another example of a study focused on the long-term effects of vagus nerve stimulation when paired with upper limb rehab, this study examined vagus nerve stimulation at 2 and 3 years post and found that motor improvements were achieved and maintained for up to 3 years post. This suggests to me that it is not just immediate neuroplasticity or recovery that may be attained in the moment, but also the potential for long-term gains in motor plasticity, not just short-term, when the vagus nerve is stimulated, or the client performs high repetition of these movement patterns.
I find these results particularly encouraging for our practice because they reinforce the idea that the neural changes we are facilitating through paired stimulation have lasting effects. When we look at the data, the durability of these outcomes highlights that the cortical remodeling occurring during these sessions is robust. It supports our role in providing intensive, high-repetition interventions, as evidence shows that the brain can retain these functional patterns long after the initial treatment phase has concluded.
VNS in Stroke Rehab
Overall, when considering vagus nerve stimulation in stroke rehab, there are a few benefits to highlight. Feedback occurs in real time because the clinician is present, triggering or stimulating the vagus nerve within milliseconds of a function-based goal-directed activity. There is also a repetitive nature to the task, which provides opportunities for motor relearning. Furthermore, the clinician can adjust the impulse as needed, using a skilled lens to decide whether a task should be upgraded or downgraded, or whether the level of challenge should be increased or decreased.
General Conclusions
The majority of the research supports vagus nerve stimulation as an adjunct to traditional therapy. However, limitations do exist, including access to resources. Of course, a medical team needs to be involved, especially given the nerve stimulation. You will need the right client who is an appropriate candidate for this type of innovative area to be used as an adjunct to traditional therapy, along with appropriate monitoring. The clinician also needs to be really well-versed in how the technology works.
As mentioned, the majority of the research is on ischemic stroke with limited evidence on hemorrhagic stroke. Additionally, the majority of the research focuses on upper extremity motor control, so limitations may include the lack of research on the lower extremities. When looking back at the chart from a few slides prior, you will see that all the examples focused to upper-limb tasks, such as reaching for an activity, grasping a cup, or grasping a spoon. When a clinician selects meaningful, goal-directed activities for their specific client, it is important to remember that research supports more upper-limb-focused activities and functional-based tasks.
I will now transition to virtual reality (VR) and augmented reality (AR), as they relate to stroke rehabilitation and more. These are also emerging areas, but these topics are often more commonly known or read about by clinicians than vagus nerve stimulation. We are in a world where VR and AR are much more common.
Virtual Reality (VR) / Augmented Reality (AR) & Stroke Rehabilitation
How do VR and AR relate to stroke rehabilitation?
Virtual Reality (VR)
To briefly describe virtual reality, it is a fully immersive and engaging experience. The real world is replaced, for lack of a better word, by headsets, and the client is fully immersed in a virtual or digital world. This is where the client can practice repetitive stimulated tasks in a virtual space. For example, a client will wear a headset and, within their fully immersive virtual space, practice buttoning a shirt.
Augmented Reality (AR)
To compare this to augmented reality, this experience is more semi-immersive but still engaging. The real world remains visible to the client. The client may use a tablet, a smartphone, or smart glasses. This is a combination of the virtual world, also called the digital world, and the real world, or the real environment the client is presently in. An example of this would be a client standing in their real-life backyard while a virtual ball is being thrown to them, and they must catch it.
Virtual Reality (VR) & Stroke Rehabilitation
Let's talk specifically about virtual reality and stroke rehab and the supporting research behind this topic.
Computer-Mediated Therapies for Stroke Rehabilitation: A Systematic Review and Meta-Analysis (Mugisha et al., 2022)
A systematic review of 22 randomized controlled trials from 2022 found that immersive virtual reality was more effective than traditional therapies in improving upper extremity function and overall ADL participation. I want to highlight one specific point here, as several terms are discussed on this slide. You will see that this review focused on immersive and non-immersive virtual reality and traditional therapies. Augmented reality was not among the terms used in this instance.
For clarity, immersive virtual reality places the client fully into a simulated environment where they are completely immersed and engaged. By definition, non-immersive virtual reality involves a virtual task displayed on a screen separate from the real environment. This is technically different than augmented reality, which integrates digital elements directly into the client’s real world. It is not always as simple as a choice between VR and AR.
This study specifically examined immersive and non-immersive virtual reality and traditional therapies. Overall, as previously mentioned, the study noted improvements in upper extremity function and motor recovery. It also demonstrated that immersive VR, where the client is fully immersed in the technology, provided greater benefits than non-immersive reality. It is important to note that both immersive and non-immersive virtual reality were found to be more effective than traditional therapies alone when promoting neuroplasticity.
One component that often comes to mind for clinicians when considering these technologies is client motivation. I want to use a specific pilot study that highlighted this as a talking point in today’s lecture. Motivation and the improvement of client motivation is important to consider, especially post-stroke, as this represents a chronic change to a client’s life and functional abilities. Clients need an appropriate level of motivation to want to use these technologies to engage their upper limb or hand function, and they may find more motivation in therapy.
MIDAS: Multi-Sensorial Immersive Dynamic Autonomous System Improves Motivation of Stroke Affected Patients for Hand Rehabilitation (Sinha et al., 2021)
One specific study I want to discuss looked at a multisensory system to improve motivation in rehabilitation. They used not only a virtual reality device but also a hand exoskeleton, and an olfactory stimulus was present. This system was designed to engage multiple senses to create a more robust user experience.
Overall, most clients reported increased motivation and found rehabilitation exciting. What the study really concluded, bottom line, was that motivation may significantly influence participation and therapy adherence. These technologies can motivate some clients, and it is really the clinician's best judgment to determine which clients would be appropriate to introduce virtual reality to and to use it as an adjunct to their therapy.
A randomized controlled trial of timing and dosage of upper extremity rehabilitation in virtual environments in persons with subacute stroke (Patel et al., 2025)
Moving on to another study focused more so with the subacute population, clinicians may ask when is the best time to use virtual reality or introduce these immersive technologies. This study focused on subacute stroke from 5 to 30 days post-infarct and found greater improvement when virtual reality was introduced 2 months post-infarct compared with 1 month post-infarct. The study emphasized that there really is no one-size-fits-all recipe for when to introduce these realities. It is really individualized based on the client's functional level, the severity of their limitations, and their motor status. As clinicians know, no stroke is the same. Every individual will have a different presentation, and we really want to consider individualization when deciding when to introduce VR.
Overall, the study found that movement quality and upper extremity function were key. For example, doing 30 repetitions of a reach or 30 repetitions of touching an inanimate object, just as a focal point, had less neuroplasticity carryover and less motor recovery than actually reaching towards a functionally based task. Quality of movement is key, goal-directed movement is key, and activity-dependent movement is key, versus just increasing the training dose alone and getting more repetitions that may not be functional.
Effects of home-based virtual reality upper extremity rehabilitation in persons with chronic stroke: A randomized controlled trial (Ase et al., 2025)
I am transitioning now to a research study that focuses on chronic stroke and the use of virtual reality, specifically at home. In this study, participants wore a virtual reality glove in their home environment. The dose and frequency of this intervention are listed here on the slide for your review. This research looked at individuals with chronic stroke, meaning more than six months post-injury, and it found that VR could be used as an effective adjunct to traditional therapy. This is particularly relevant for individuals with chronic stroke who may have been discharged from formal therapy or who may be working on their home programs between sessions in an outpatient setting.
The researchers used the Fugl Meyer, the Motor Activity Log, the Box and Blocks Test, and the Jebsen-Taylor Hand Function Test, and found improvements across those assessments. Again, home-based virtual reality could be an option to promote increased meaningful movements and upper extremity functioning. It allows us to engage clients in activity-dependent upper-limb movements at home when they are not necessarily in the clinic with a therapist. Virtual reality can serve as a tool to promote carryover and self-management beyond the clinic, and this article provides the research to support that use. Later, after we discuss augmented reality, I will talk about its limitations and how to identify the right client for this technology. For now, this serves as evidence in support of this emerging area as I transition into augmented reality and stroke rehabilitation. Remember, augmented reality is a semi-immersive reality device.
Augmented Reality (AR) & Stroke Rehabilitation
How can augmented reality be used in stroke rehab?
Effectiveness of Augmented Reality in Stroke Rehabilitation: A Meta-Analysis. Applied Sciences (Phan et al., 2022)
A 2022 meta-analysis examined comparisons between upper extremity and lower extremity recovery and motor control, specifically with augmented reality. The results supported significant improvements in upper extremity function, motor recovery, and neuroplasticity, while only a moderate effect was noted in the lower extremity. This study also highlighted an increase in engagement and motivation when compared to traditional therapy alone. Using augmented reality as an adjunct to traditional therapy was found to be more effective in promoting both motivation and motor recovery.
The study also highlighted limitations that I believe apply to both virtual and augmented reality devices. Some components that I really want you to consider from a limitation standpoint include any vestibular needs or concerns the client may have. This study specifically pointed out the possibility of simulator sickness. When a client is in immersive or semi-immersive environments, they may experience simulator sickness if they have underlying vestibular concerns.
There also needs to be consideration of depth perception if your client has any limitations or needs, especially regarding upper-extremity reaching and the engagement of the upper limb in functional tasks. Lastly, because augmented reality is semi-immersive, the client's real environment remains present, making environmental considerations key. From a safety and fall-prevention perspective, I want to ensure we guide our clients in a very safe environment when using these devices.
Impact of the Combination of Virtual Reality and Noninvasive Brain Stimulation on the Upper Limb Motor Function of Stroke Patients: A Systematic Review and Meta-Analysis
(Zhang et al., 2024)
Transitioning to another article I want to highlight, this systematic review and meta-analysis from early 2024 examines the combination of virtual reality with non-invasive brain stimulation. I selected this as a talking point today because it provides a nice overview of how the emerging areas we have discussed can actually intersect. Specifically, this study examined upper-limb motor function in patients with CVA and found that the combined effect of virtual reality and non-invasive brain stimulation was stronger than either VR or brain stimulation alone.
The study noted that the stimulation was targeted at the motor cortex. While it did not specifically focus on the vagus nerve stimulation we discussed earlier, it still highlights the power of a brain stimulation component in combination with virtual reality. As clinicians, we can start to see how these two emerging areas—vagus nerve stimulation and virtual or augmented realities—might be combined. This systematic review introduces that very idea, reiterating that the combination of treatments resulted in significant improvements in upper extremity motor control compared to either modality used in isolation.
What this suggests for our practice is that as these technologies continue to evolve, we may see more protocols that leverage the "window of plasticity" created by stimulation while simultaneously using VR to provide the high-repetition, goal-directed tasks necessary for cortical re-mapping. This dual-intervention approach seems to offer a more robust recovery pathway than a single-modality approach.
So it's starting to look at a combination of these emerging areas.
Functional Implications and Practicality
Some of the benefits of using these emerging areas, per the study that examined both virtual reality and non-invasive brain stimulation, include real-time feedback. Because these are technology-based interventions used as adjuncts to traditional therapy, the technology component enables real-time feedback, enabling immediate decision-making by both the clinician and the patient. These systems are immersive, which can lead to higher levels of motivation and engagement for some clients.
The movement patterns the client engages in should be goal-directed and activity-dependent, which aligns perfectly with our role as occupational therapists. Additionally, the technology emphasizes repetition and motor relearning within functional tasks. The opportunity to adjust the activity's challenge or movement occurs in real time. With virtual reality and vagus nerve stimulation, there is the technology aspect, but when guided by a clinician, the therapist can use their skilled lens to make adjustments for task gradation as needed.
Overall, there are several functional implications for virtual and augmented reality, as well as for vagus nerve stimulation. First, these emerging areas should be used as adjuncts to traditional therapy. The research supports this, and these tools will never replace the OT's role. The second implication is compliance. As a clinician, you want to introduce these technologies to clients who you feel will be compliant. Clients may be more motivated to engage in their home programs or to use their upper limbs in functional tasks when using these technologies, but you must make an individualized decision for each patient. The client should also have a baseline level of volitional motor control to engage in functional tasks, such as grasp-and-release or functional reach.
We must also weigh cognitive considerations, such as the ability to follow simple to multi-step directions, as well as safety perspectives, decision-making, and judgment. Vestibular considerations are also vital. Because simulator sickness was highlighted as a primary limitation, you must assess the severity of any vestibular concerns before introducing reality systems, goggles, or tablets.
Lastly, motivation can be addressed in several ways. A client who enjoys cutting-edge technology may be very motivated to try virtual or augmented reality. In other cases, seeing their motor recovery in real time within an immersive environment can produce more intrinsic motivation. Conversely, some clients may prefer traditional therapy and may lack the motivation to use these devices. While you may be excited to try these technologies, it is important to look at the client's motivation. One study specifically focused on how virtual reality can be used in chronic stroke when the client is not in the clinic, either as an adjunct to a home program in an outpatient setting or after discharge to carry over motor relearning.
Relation to the OT Practice Framework
Now let's discuss these emerging areas in relation to the OT practice framework (OTPF).
Motor Skills
Starting with motor skills, we look at the specific categories listed in the OTPF. One of the primary areas I want to address is posture, which includes positioning and stability. Many of the studies we have discussed focus on upper extremity motor recovery, and, as clinicians, we often follow the principle of proximal stability to enhance distal use. We must ensure the client has the trunk control and balance necessary to engage in functional reaching.
This leads us into the mobility category, specifically reaching and bending, and then into fine motor skills like coordination and manipulation. This is where a client’s motor levels should be assessed through a functional lens. As a clinician, you must determine their baseline motor recovery: What are their volitional abilities to grasp, release, and engage in functional reach?
Other areas per the OTPF include strength, effort, and energy. Because high levels of repetition are essential when using vagus nerve stimulation or virtual and augmented reality devices, we are not just looking at motor recovery; we are also looking at endurance. "Endures" and "paces" are two subcategories we must assess, as the high-frequency repetition requires significant physical and cognitive energy from the client.
Client Factors
There are also client factors to consider, specifically mental functions such as attention, memory, and orientation. This is especially true with virtual and augmented reality. When clients are in fully immersive or semi-immersive environments, we have to monitor their orientation; we don't want a client to become disoriented or confused, as significant safety concerns can arise from that.
In terms of sensory functions, I have highlighted vestibular needs and considerations quite a bit already from a simulator sickness perspective. Proprioception is another area that is highly activated when clients engage in reaching-based activities, especially in a virtual space where they must perceive their limb's position without the same tactile feedback as in the real world.
Finally, we must look at neuromusculoskeletal and cardiovascular functions. This relates back to the "endures" and "paces" categories—the client's actual endurance to engaging in highly repetitive movements or functional tasks. These technology-based interventions are intensive, and the client's physiological capacity to sustain that effort is a key factor in their success.
Individual Factor Considerations
Clinicians should assess several key areas to ensure the safe and effective engagement of their clients with virtual and augmented reality, as well as vagus nerve stimulation. There are specific considerations to determining whether your client is an appropriate candidate, beginning with pain levels and any complicating diagnoses or comorbidities.
We also need to look at levels of spasticity or tone. There should be a baseline level of volitional movement, and it is truly the clinician's judgment to determine this based on the specific functional task they decide the client should engage in while using these emerging areas as adjuncts to therapy.
Other critical factors include client motivation, cognition, motor control, trunk control, and joint stability. While we have highlighted some of these already, this comprehensive list serves as a reminder that these are individualized decisions. As clinicians, we must make these calls based on how our specific client is functioning and presenting in the moment.
Area of Occupation
It's important to remember that augmented reality, virtual reality, and vagus nerve stimulation should be used for activity-focused, activity-dependent tasks. It is occupation-based. Areas of occupation per the OTPF may include bathing or showering simulation, dressing the upper and lower body, functional-based tasks, functional mobility or reach, caring for others, health management or maintenance, meal preparation and cleanup, and leisure participation.
These are areas within the OTPF that could be addressed using these emerging areas as adjuncts to our therapy approaches. When we select these tasks, we ensure that the neuroplasticity we promote through technology is directly translated into the functional roles that matter most to our clients.
Daily Activities
Additional daily activities include reaching overhead to style hair, reaching behind the back for perineal care, lifting during household chores, loading or unloading groceries, and donning and doffing shoes.
As mentioned earlier, buttoning was a key example used in one of the studies. I also highlighted this when showing the chart for vagus nerve stimulation: reaching for a hat, with the nerve stimulated the moment the hand touches the object. If we are discussing unloading groceries, the vagus nerve could be stimulated exactly when the hand comes into contact with the fruit being moved from the grocery bag into the refrigerator.
These examples reinforce the necessity of timing the stimulation to a specific, functional goal. Whether it is styling hair or handling groceries, the pairing of the electrical pulse with the exact moment of task achievement is what drives that activity-dependent neuroplasticity we are looking for.
Task Analysis and Activity Breakdown
Our clinical lens as skilled clinicians is key, and we would want to ask ourselves: Does the client present with a baseline level of appropriate motor control of the upper limb? Specifically, which individual movements occur at each joint for the client to effectively engage in the occupation or activity?
What is the motor control, range of motion, or baseline strength at the shoulder, elbow, wrist, forearm, and fingers? This is where our skilled lens of activity analysis and activity breakdown really come into play. We are not just looking at the movement as a whole, but assessing the components required for success. For example, does the client have the shoulder flexion and elbow extension necessary for a functional reach, or the wrist stability and finger isolation required for a pincer grasp?
By breaking down these movements, we can determine the exact moment to trigger vagus nerve stimulation or how to grade a virtual environment to meet the client's current abilities. This ensures that the intervention remains focused on the specific motor deficits preventing independence in daily occupations.
Preparatory Measures
Preparatory measures remain a cornerstone of our practice, even when incorporating high-tech adjuncts such as virtual reality or vagus nerve stimulation. These emerging areas do not replace the foundational work required to prime the body for movement; they build upon it.
If your clinical reasoning indicates a need for modalities, stretching, or passive range-of-motion activities to reduce stiffness or prepare the joint for action, these should still be completed first. This ensures that when the client enters the virtual environment, they have the maximum available range for motor engagement and participation.
Similarly, the client’s balance must be assessed and prepared. Before a client ever dons a headset to engage in dynamic reaching, we must ask: Do they have the baseline postural stability to remain safe? If not, preparatory balance training—such as core activation or weight-shifting exercises—is necessary to provide the "proximal stability" needed for "distal mobility" in the virtual space.
I also like to highlight breath work as a vital preparatory measure. Focused breathing can have significant implications for managing tone and spasticity. By calming the nervous system through diaphragmatic breathing, we can potentially lower overall hypertonicity, making it easier for the client to achieve the volitional movement patterns required by the technology.
Frames of Reference
So I think those are some great preparatory measures to remind ourselves, as clinicians, that we do want to continue with what we would traditionally do in our therapy, and then use the innovative areas as adjuncts to the frames of reference as OTPs. When using these technologies, we would consider a biomechanical frame of reference and motor learning theory.
Summary
So, let’s bring this all home. We’ve spent today wandering through the digital woods and the frontier of neural stimulation, but we have to ground this in reality by acknowledging that limitations are very real. When we talk about vagus nerve stimulation, we aren't just talking about a cool gadget; we’re talking about a significant medical intervention. Whether it’s the implanted version or the non-invasive skin-surface approach, you are part of a high-stakes team. You will be working alongside neurologists and surgeons, and you have to ask the hard questions: Does your facility have the infrastructure? Does your client have the medical clearance? And let's be honest—is the client’s insurance even ready to cover this?
Then there is the virtual and augmented reality side of the house. Beyond the technical glitz, there is a very real wall called cost and coverage. These devices aren't cheap, and the software is often specialized. We have to be the advocates for our patients to ensure they have access to these tools, whether they are in our clinics or trying to manage a chronic stroke at home.
If you take nothing else away from today’s lecture, remember that the research is detailed: these technologies are a powerhouse for upper-extremity recovery.
While we see some moderate wins for the lower limb, the real magic happens from the shoulder down to the fingertips. The research supports that VR, AR, and VNS are not just fancy add-ons; they are high-octane fuel for neuroplasticity when paired with traditional therapy.
Finally, a word of caution to the repetition-obsessed: quality of movement is everything. Yes, the technology helps us hit those high numbers, and we definitely want those hundreds of reps. But three hundred bad, compensatory reaches are just teaching the brain how to move poorly. Our job as occupational therapists is to use our skilled lens to ensure that every single rep—whether stimulated by a pulse or performed in a headset—is a high-quality, goal-directed movement.
You are the architect of the just-right challenge. You set the stage, you grade the task, and you ensure that the technology is serving the occupation, rather than the other way around. We aren't being replaced by robots; we are just getting better tools to do what we have always done: helping people reclaim their lives.
Questions and Answers
Does VNS require specialized training for clinicians?
Yes. VNS involves stimulating a specific nerve in a very precise way, which requires the clinician to be fully versed and competent in the technology. It is not a tool you can use without extensive understanding and training.
Who oversees the implementation of VNS therapy?
It is a collaborative effort. While therapists provide input, you must work closely with a medical team and physicians. For invasive VNS, the medical team makes the final decision on its use.
Where is VNS typically administered?
Because of the medical oversight required, VNS is usually found in facilities with close ties to medical centers or physician teams rather than in general "layman" environments.
How does the accessibility of VR/AR compare to VNS?
VR and AR are much more accessible. You often see them used in non-rehabilitative settings (like gaming glasses or tablets), so they are more common in the layperson's environment outside specialized rehab centers.
Can VR/AR be used in settings like nursing homes?
Yes, but it is an individualized decision. While there may be specific site or location limitations, the clinician must determine if the technology is appropriate for the specific client.
How does VR/AR fit into a standard therapy session?
These technologies are used as an adjunct to functional tasks. For example, a patient might practice the mechanics of buttoning a shirt in a virtual environment before or alongside physical practice.
Does the patient's age impact the effectiveness of these treatments according to the studies?
The current research focuses less on the patient's age and more on chronicity post-stroke. The studies generally categorize participants by the time elapsed since their stroke: Subacute stroke (5 to 30 days post-stroke) and chronic stroke (More than 6 months post-stroke).
I hope you had some great takeaways from today's lecture. Thank you so much.
References
See additional handout.
Citation
Dimopoulos, T. (2026). Stroke rehabilitation: Vagus nerve stimulation and virtual and augmented reality. OccupationalTherapy.com, Article 5866. Retrieved from https://OccupationalTherapy.com
