Editor's note: This text-based course is a transcript of the webinar, Elevating OT Fieldwork Education, Foundations, Theory And Practical Strategies, presented by Elizabeth DeIuliis, OTD, MOT, OTR/L, CLA, FNAP, FAOTA.
*Please also use the handout with this text course to supplement the material.
Learning Outcomes
- After this course, participants will be able to recognize the educator component within the OT/OTA Role.
- After this course, participants will be able to explain how OT beliefs, values, and principles align with key teaching and learning theories.
- After this course, participants will be able to describe strategies to enhance student clinical reasoning and learning within your own practice as a fieldwork educator (FWed).
Introduction
Welcome to today's session. I have been an occupational therapist for over twenty-one years. I have been a full-time faculty member in higher education for more than sixteen years, and prior to that, I was a very active and dedicated fieldwork educator in practice. Adult acute care is my clinical area of practice and expertise, and I have also held administrative roles in developing clinical fieldwork programs. I served as an academic fieldwork coordinator for over ten years and, more recently, as a program director in a dually accredited master's and doctoral program. Although I no longer manage the nuts and bolts of fieldwork in my day-to-day role, it remains a very important part of my passion and professional interests as an occupational therapist and educator.
I truly feel that fieldwork is the most transformative experience in an occupational therapy student's journey, and that is because of the selfless dedication of our fieldwork educators, who step up and choose that role to mentor and educate students. However, fieldwork is not always rainbows and butterflies. There can be a steep learning curve in becoming an effective fieldwork educator or some hiccups along the way. I think it is important to share that being an experienced or expert clinician does not automatically mean that you are going to be an expert fieldwork educator. The reality is that there is a skill of teaching skills and, more specifically, a unique skill set to teach clinical skills. This requires unique strategies, patience, and intentional practice, which is the focal point of today's session.
We are really digging into the concept of being an intentional fieldwork educator and learning to think like an educator in that role. In this session, we will recognize the educator component of the therapist and assistant roles. Being a clinician or practitioner is just one aspect of explaining how core occupational therapy beliefs, values, and principles align with key teaching and learning theories. There is significant alignment and synergy between occupational therapy and education. Lastly, I hope to provide you all with plug-and-play teaching tools you can implement in your daily practice as fieldwork educators to promote student clinical reasoning and learning.
Thank You For Being Here
I would first like to thank you all for being here. As both a former fieldwork educator and academic fieldwork coordinator, I fully understand and give deep appreciation to the fact that serving as a fieldwork educator is an add-on. There is typically nothing coming off your plate or being reduced from your workload to serve as a fieldwork educator. Being a fieldwork educator is a significant role and responsibility that takes time, energy, and commitment. It is a balancing act to do it effectively.
I hope that this course helps to reframe the concept that being a fieldwork educator is just extra work. Instead, I invite you to think of it as a professional contribution that not only shapes the future of the occupational therapy profession but also your own personal and professional development as an occupational therapy practitioner.
Objective 1: Recognize the Educator Component Within the OT/OTA Role
We are going to jump into content related to our first objective: recognizing the educator component within the occupational therapist and occupational therapy assistant roles. It is vital to understand that our identities as practitioners are inherently tied to our identities as teachers. When we transition into the fieldwork educator role, we are not simply adding a task to our list; rather, we are expanding upon the pedagogical foundation that already exists within our clinical practice. Each interaction with a student extends the therapeutic education we provide to our clients every day.
OT Roles
When we look at the occupational therapy role broadly, we see that it comprises several components. We wear a lot of hats. The roles we use clinically might include practitioner or clinician, but we also act as advocates, researchers, and managers. That educator piece is a fundamental component of this overall role we hold.
Outside of being a formal fieldwork educator with students, we wear that educator hat in a variety of ways in clinical practice. We educate, instruct, teach, and train our clients, families, and caregivers. We also educate and instruct members of our interprofessional teams at our work settings. Whether it is teaching a nursing assistant safe body mechanics for moving and handling, or instructing a speech-language pathologist on safe biomechanical positioning to influence a person's arousal during the occupation of self-feeding, we are constantly teaching. We also educate volunteers or other students within our work environments.
Reflective Question
These reflective questions are intentionally designed to give you a moment to pause to think, and reflect. If you have a piece of paper nearby, I encourage you to jot down any thoughts or ideas that come to mind. Reflective questions are a vital part of the teaching and learning process. It is what helps us make sense of experiences, connect ideas, and deepen our understanding.
The first reflective question is: What are the ways in which you teach your patients or your clients in practice? Consider the specific methods, the verbal cues, or the demonstrations you use as you navigate those clinical interactions.
Ways in Which We Teach in Practice
So what do you do? How do you do that? How do you teach? What are some things that you do? Just take a moment and think about that. In practice, we utilize a variety of approaches that center on teaching our patients, clients, families, caregivers, and interprofessional team members. For example, we teach by demonstration. Perhaps you are working with a client who just had a total hip replacement, and you may demonstrate to them how to use the sock aid as part of their movement precautions. We teach by cueing or prompting. To work on metacognition and self-awareness in a client with a brain injury, we might use strategies such as guided discovery or fading different types of cues and prompts to support skill acquisition and learning.
We might use literature or media, such as patient education materials, to support learning and carryover for our clients. The reality is, we use different strategies to teach and instruct based on the person, the client, the occupation or activity we are focusing on, and the client's overall goal. What we do not necessarily spend a lot of time on in the classroom as students, or even in practice when engaging in other professional development or continued education, is focusing on the best way to teach or instruct a client to do things. Here is the gap we hope to fill in for you during this session. We will explore best-practice approaches to foster effective learning specific to students during fieldwork education.
Being a Fieldwork Educator is Part of Being an OT
If we take a closer look at the 1993 AOTA role paper, we can further unpack this occupational therapy role to include the fieldwork educator role. All of these resources and references are in the reference list, and I encourage you to take a closer look. We are informed, even as students, that fieldwork serves as a bridge. We have all heard that metaphor before. It serves as a bridge between the classroom and the clinic, and we really rely on the fieldwork educator role to help students navigate it. The question remains: What training or resources are provided to support the teaching expectation of being a fieldwork educator?
Fieldwork Educator (FWed)
The fieldwork educator role is a term intentionally used in occupational therapy. This is the specific language we use, not fieldwork supervisor or clinical instructor, although those might be terms adopted by other professions. That is not our jargon in occupational therapy.
So why do we use the term fieldwork educator? This choice helps shape the professional identity of this very important role. By including the word' educator,' we emphasize that practitioners supervising students are not merely supervisors. They play an active, intentional, professional role in teaching and shaping future occupational therapy practitioners.
This fieldwork educator term also highlights the partnership and the collaboration between occupational therapy academic programs and practice settings. Both are equal parts of a student's education. Again, that educator term aligns with what is used in adult learning theories. It also demonstrates our commitment to teaching through modeling, guided practice, and reflection. Lastly, the term fieldwork educator is deliberately used and adopted by our professional organizations in occupational therapy.
Role Competencies of Being a FWed (AOTA, 2006)
The American Occupational Therapy Association and the Accreditation Council for Occupational Therapy Education both use the fieldwork educator term to align with educational outcomes and accreditation language. In 2006, the American Occupational Therapy Association published a white paper titled "Role Competencies of Being a Fieldwork Educator." It framed out five competency areas of the fieldwork educator role. These competencies are designed to holistically describe the values, knowledge, and responsibilities that are needed to be successful and effective in the role.
Firstly, we have knowledge. You must understand what it means to be a fieldwork educator, be able to develop learning activities, and understand the teaching and learning process. Second is critical reasoning. You have to be able to integrate theory and evidence, and model and communicate it to students. Third is interpersonal skills. This involves having a positive attitude towards mentoring and the fieldwork educator role while being able to advise, guide, communicate appropriately, and provide feedback to students. Fourth is performance skills. This includes being able to develop and modify learning objectives and learning experiences, evaluate student performance, and document progress. Lastly, we have ethical reasoning, which involves being able to serve as a role model and an advocate for the student.
These competencies help us understand that the fieldwork educator role is both a practitioner and an educator. That role requires mastery of clinical skills along with the ability to teach, evaluate, communicate, and reflect within that academic and practice partnership with your student. The American Occupational Therapy Association Fieldwork Certificate Workshop has been available since 2010 and is a fabulous professional development opportunity. This training really focuses on advancing skills around the supervision, administrative, and evaluation parts of the fieldwork educator role, which are certainly very important. However, that workshop does not necessarily dig into specific ways to improve the educator component of the fieldwork educator role.
Let's look at our next reflective question.
Reflective Questions
Let us pause and reflect on how you were socialized to the fieldwork educator role. How did you come to know about it? Perhaps it happened in the classroom during your formal occupational therapy education. Maybe it was on-the-job training, or perhaps you tapped into your own personal experiences as a prior fieldwork student.
Depending on when you entered practice, you might have had specific training in the classroom to prepare you to serve as a fieldwork educator, while others might not have had that same experience.
Snapshot of OT Educational Standards (ACOTE)
Here is a quick snapshot of how accreditation standards for teaching and learning, specifically for educators preparing for fieldwork, have evolved. Ten to fifteen years ago, under the 2011 standards, occupational therapy and occupational therapy assistant programs were actually expected and required to teach their students about the fieldwork educator role. All programs were required to demonstrate compliance with that standard.
As the language for accreditation standards evolves roughly every five years, new academic standards are adopted and enforced. The specific standard about preparation to serve as a fieldwork educator has been removed. Programs do need to meet these other standards, which certainly hit certain notes about teaching and learning, but programs can interpret and respond to them in different ways. In regards to socializing our future fieldwork educators, who are basically our current students in many ways, their exposure to the role and their understanding of different supervision or clinical teaching strategies is generated by their experience with you all as their fieldwork educators.
The takeaway here is that some programs might still emphasize fieldwork educator development in their curricula, while others might not. As fieldwork educators, you can help students prepare for that future role by modeling best practices, being evidence-based, and demonstrating your own lifelong learning perspective. I always like to mention that during Level 2 fieldwork experiences, there is an opportunity for a student to test the waters and help with the instruction of volunteers or other students at your work setting. These can be great ways to grade up Level 2 fieldwork objectives, especially for that exceptional student.
Moving on to our next question, I will preface it by noting that, as occupational therapy practitioners, we are trained to observe and understand the relationships among a person, the environment, and occupation. We examine how those three constructs interact to support performance. That is a core concept in occupational therapy, and it allows us to be person-centered, context-sensitive, and to support meaningfulness in our role as practitioners.
Reflective Question
With that context in mind, the next question I would like you to consider is: what contextual factors are at play in your environment that influence or impact how you teach, supervise, and support fieldwork students? Take a minute to think about that. Consider what is happening around you in the different contexts where you interact as an occupational therapist and as a fieldwork educator. What are the things that impact and influence that process?
As we reflect on these factors, we can see how they naturally align with our professional models. For instance, the environment might involve the fast-paced nature of an acute care setting, the physical layout of your clinic, or even the institutional culture regarding student education. The person aspect involves both your own teaching style and the student's unique learning needs or prior experiences. Finally, the occupation in this scenario is the act of clinical reasoning and therapeutic intervention itself. Understanding how these elements intersect helps us identify why some days feel seamless while others present more of a challenge in the educator role.
Consideration of Context and Influential Factors in Fieldwork
We are going to look at some context and influential factors here relative to fieldwork. Certainly, your work setting is a primary factor. These can include factors related to the setting you work in, the patient population you serve, and the general demands of working there, such as caseload and productivity requirements. On the fieldwork side, it is helpful to have a student manual on-site, along with site-specific learning objectives that outline expectations and define entry-level performance. Defining entry-level competence could be a whole separate course in itself, but it is indeed something defined by the site and the fieldwork educator.
You may affiliate with different academic programs, and different programs are going to have different fieldwork models. This is especially true for level one fieldwork, where programs have greater latitude and flexibility in designing and delivering those experiences. You might interact with programs that use a block model, in which fieldwork occurs within a designated timeframe, such as one or two weeks at the end of a semester. Alternatively, they might use a dose model in which a student comes to you every Tuesday throughout the semester. Along with these differences in structure come different assignments or evaluation measures that you need to be knowledgeable of. Many occupational therapy and assistant programs are now adopting clinical databases that you might need to interact with as a fieldwork educator or clinical coordinator.
Then, of course, we have the student. They bring a range of unique factors that influence fieldwork, including their learning styles, life experiences to and specific academic preparation. All of these elements, the site, the program, and the student, interact within the environment of the fieldwork experience to shape how teaching and learning occur.
Generational Stereotypes of Gen Z (Roughly born 1997-2012)
We can look at this from a generational perspective. With generational theory, cohorts are often described as having stereotypical strengths and areas for growth. Our typical college-age students right now generally fit into Generation Z, but you might also accept a fieldwork student in a non-traditional academic pathway. They could be a second-degree student who falls into another generational category.
As a fieldwork educator, being mindful of generational preferences is important because these factors influence communication styles, interactions with authority, work ethic, and learning styles. Is this something you intentionally make a point to obtain from your fieldwork students? Do you use a learning style inventory, or do you get a baseline of their hard and soft skills? These are crucial things to seek out as your student's educator in the clinic because you will use this information to individualize and personalize your teaching. Within the fieldwork educator role, your student is essentially your client, and you need to be student-centered and holistic. You cannot have a cookie-cutter approach. You cannot do the same thing the same way with every student. We already operate this way with our patients; we understand that no two individuals with a stroke present the same way, and we need to apply the same logic as educators.
To dig a little deeper into generational stereotypes, the majority of our current students are Generation Z. While Baby Boomers are often called Boomers, Generation Z is nicknamed Zoomers to reflect their engagement with the web and virtual environments. It is predicted that Generation Z will account for 30% of the workforce by 2030, which is not far away. This will be the demographic of your coworkers in the very near future. These are stereotypes based on the formative years of those individuals and what was happening in the world around them. Instead of saying strengths and weaknesses, I prefer a strength-based approach using glow and grow areas. Glow areas are ways this generation excels, and grow areas are those that may be underdeveloped.
Generation Z members are digital natives. They understand technology and are super efficient and productive with it, but the flip side is that they are sometimes described as tech-dependent. This generation can be extremely innovative and individualistic. They are primed to be self-advocates, but that can sometimes be perceived as entitlement or a lack of self-awareness and coping skills when things get tough. Understanding these characteristics helps you tailor your communication, supervision, and teaching strategies to our students' needs and preferences. These efforts are purposeful to create more engaged learning experiences, foster stronger professional relationships, and support clinical reasoning.
Consideration of Context and Influential Factors in OT Education
Now, let's look at the classroom context from the other side of the bridge. An important component of fieldwork is its partnership and collaboration between the fieldwork site and the occupational therapy academic program. Let us look at some of those influential factors. Institutionally, programs have the expectation to align their education and student learning experience to the mission, vision, and identity of the institution. As a fieldwork educator, what is your comfort level and confidence level regarding the different universities or programs that you collaborate with?
At the program level, each has its own unique philosophy, curricular design, scope, and sequence. Based on the number of programs you affiliate with, how comfortable are you in articulating and understanding those unique qualities within each program? At the professional level, our national organization, the American Occupational Therapy Association, provides broad guidelines to support education and fieldwork. If you are not familiar with the philosophy of occupational therapy education white paper, I am going to give you a broad overview on the next slide. This is a source included in the references, and I highly encourage you to look into this document further.
The philosophy emphasizes that education is a collaborative process and that students should be active participants in their learning. It highlights the importance of professional reasoning, critical thinking, and the integration of theory and practice. Understanding this framework helps us see that the academic side is setting the stage for the practical application you provide in the clinic.
Philosophy of OT Education (AOTA, 2018)
When you look at the Philosophy of Occupational Therapy Education, which is also updated roughly every five years, you see that it outlines the fundamental beliefs and values of occupational therapy education and programs.
Programs use this as a guide to frame their own unique program philosophy and curricular design. As a fieldwork educator, I believe this document provides a useful starting point to think about occupational therapy education in general. As I mentioned before, in your role as a fieldwork educator, your students are your clients. The classroom is the fieldwork setting. The anticipated outcome is that you want your student to develop entry-level competency and overall workforce preparation.
Even as educators, we commit to embracing a lifelong learning perspective. As clinicians, you are expected to engage in regular professional development and continued education to keep your clinical skills sharp, advance your knowledge, and maintain your credentials. As educators, we have that responsibility too. We are continually developing the art and craft of our teaching approach.
Consideration of Context and Influential Factors in OT Education
And, of course, we have the Accreditation Council for Occupational Therapy Education, which accredits our education. They set the standards that outline the minimum requirements for each degree level. This guides both the administrative and curricular components of occupational therapy education, and it includes standards that relate specifically to fieldwork. A lot of them are for the academic fieldwork coordinator to ensure that the program is in compliance. However, I think it is important that you take a look at those standards, which you will see listed as the C standards, because they provide a lot of rationale for the very specific communication and collaboration that is driven by the academic program prior to, during, and after fieldwork experiences.
Lastly, we have educational best practices grounded in teaching and learning theories. Understanding these theories allows us to move beyond simply supervising and toward truly educating. When we look at how a student acquires a skill, we can see the transition from novice to expert as a structured process rather than a random series of events. By leaning into established educational frameworks, we can better troubleshoot when a student is struggling and provide the right level of challenge when they are excelling.
Teaching and Learning Theoretical Frameworks
Within the theoretical frameworks of teaching and learning, there are two main schools of thought. There is pedagogy, which refers to the teaching and learning process with children. This is typically what you see in kindergarten through twelfth-grade education. Then there is andragogy, which refers to adult learners. As occupational therapy and fieldwork educators, we want to tap into teaching and learning theories that align with our student audience, who are adult learners.
Adult learners bring a different set of motivations and life experiences to the table compared to children. They are typically self-directed, goal-oriented, and need to understand the relevance of what they are learning to their future roles. Understanding these distinctions allows us to move away from a top-down instructional style and toward a collaborative mentorship model that respects the student’s autonomy and prior knowledge.
Conceptual Frameworks
Conceptual frameworks are not unfamiliar to us as practitioners. As clinicians, you might not intentionally think about each of these in your daily practice, but with your expertise, you are subconsciously using principles within these theories and frames of reference to maximize your client outcomes. These conceptual tools help structure your decision-making, guide your intervention planning and selection, and support your clients in achieving meaningful occupational performance. Even if the terminology feels unfamiliar, the strategies and approaches that you use daily are grounded in these theoretical frameworks, making them an integral part of effective occupational therapy practice.
The same holds true as you transition into the educator role. Just as you use a frame of reference to guide a client through a stroke recovery, you can use educational frameworks to guide a student through clinical reasoning. You are already doing the work of an educator; we are simply putting names to the tools you are already using.
Objective 2: Explain How OT Beliefs, Values, and Principles Align With Key Teaching and Learning Theories
This is a great transition into our second objective, where we are going to dive more into understanding how certain teaching and learning theories have a direct connection to occupational therapy beliefs, values, and principles. Just as we use models of practice to understand our clients, we can use these educational frameworks to understand our students.
The transition from clinician to educator is often most successful when we realize that the skills we already possess as therapists are the same skills needed to be effective teachers. By making these connections explicit, we can move from a subconscious style of instruction to a more intentional and evidence-based approach to fieldwork education.
Adult Learning Theorists
Relative to occupational therapy theories and frames of reference, you might be referring back in your brain to Jean Ayres, the Bobaths, or Gary Kielhofner, the pioneer of the Model of Human Occupation. These are all pioneers and scholars who developed occupational therapy models of practice and clinical intervention frameworks. In education, theorists have developed concepts that have promoted best practices in teaching and learning. I am just going to highlight a few of them. Certainly, this is not all-encompassing, but we will start with Benjamin Bloom. He is best known for developing Bloom's taxonomy, a framework to understanding and structuring learning.
Bloom's taxonomy provides a hierarchy that moves from foundational knowledge to higher-order thinking. When you are working with a student, it is helpful to identify where they are on this pyramid. Are they at the beginning stage of just remembering and understanding the steps of a transfer, or are they moving into applying and analyzing that information in real time with a complex patient? Understanding this progression allows you, as a fieldwork educator, to set appropriate expectations and provide the right type of challenge to further develop their clinical reasoning.
Learning Outcomes/Bloom's Taxonomy
The taxonomy focuses on cognitive levels, from simple recall of facts to higher-order thinking and knowledge synthesis, as well as learning that involves cognitive, emotional, and behavioral components. As educators, we rely heavily on Bloom's taxonomy to develop clear, measurable learning objectives.
Learning objectives are specific statements that describe what a learner is expected to know, understand, or be able to do by the end of a lesson, course, or learning experience. Learning objectives guide both the teaching and assessment. They help educators design activities and evaluate whether students have achieved the intended outcome. Think of these like goals. In clinical practice, we know that for goals, we want them to be specific, measurable, relevant, and time-bound. We should use the same approach to craft learning objectives for occupational therapy students' fieldwork, both in the classroom and in the clinic.
Figure 1 shows a nice visual of Bloom's taxonomy.
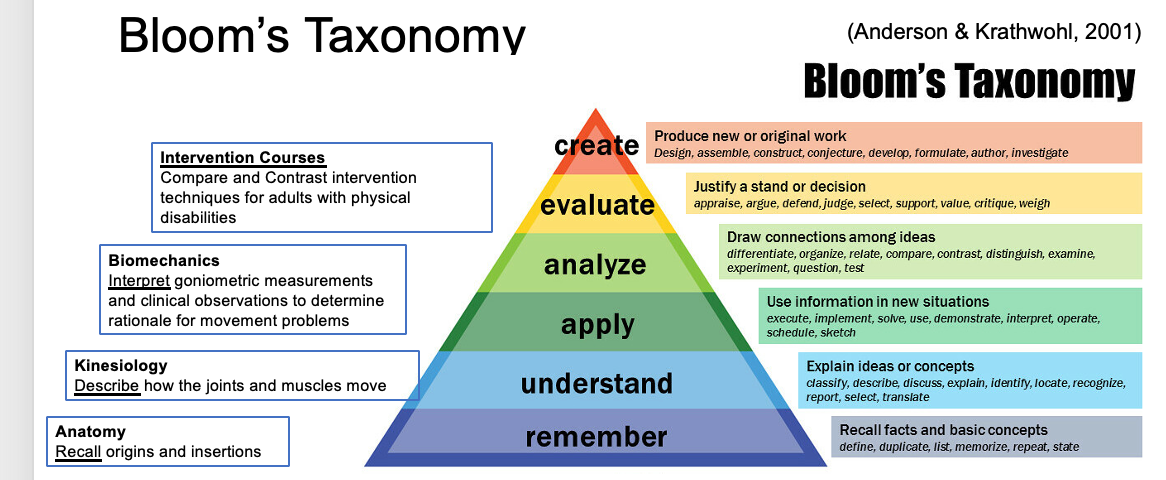
Figure 1. Bloom's Taxonomy. (Click here to enlarge the image.)
It is a hierarchy with lower levels of knowledge at its base. These emphasize foundational content. Think about it in terms of recalling facts and concepts. In occupational therapy education, we might think of a foundational course, such as anatomy, where students are expected to recall, memorize, or list the origins and insertions of muscle groups. From there, a student might progress to a kinesiology course where they are expected to apply the knowledge they have previously learned in anatomy to understand and explain concepts. Now the learning objective is to describe how joints and muscles move or to discuss and explain those mechanics.
From here, you might progress to a biomechanical clinical course where students draw conclusions and interpret goniometer measurements and clinical observations to determine the rationale behind movement patterns. Then it may develop into additional intervention courses in which students are expected to compare and contrast intervention approaches for adults with physical disabilities. This gives you an idea of how learning and knowledge are built and scaffolded. Scaffolding is a really important term in the education world, referring to the ability to connect knowledge and learning.
In this diagram, each level of knowledge provides verbs for educators to use when designing learning activities. It is important to understand that, within this hierarchy, we cannot expect students to perform at one of the upper levels without having success at the lower levels. That gives you some good food for thought. For example, if you have a level one fieldwork student who has not yet taken a kinesiology course, we cannot expect them to jump ahead to comparing and contrasting interventions because they have not yet mastered the foundational content.
Site-Specific Learning Outcomes
In fieldwork education, we want to establish site-specific learning objectives. This is used to provide clear expectations so students know exactly what knowledge, skill, or behavior they are expected to demonstrate. This is really important because it helps to promote transparency within the learning experience, which also helps to reduce student anxiety and promote their accountability. Providing site-specific objectives also allows the student to have measurable benchmarks to allow them to engage in self-reflection on their own progress, to identify their strengths, and to target those areas for improvement. It also helps you, as the educator, to be able to anchor your supervision and evaluation in their performance.
We are not going to go further into designing site-specific learning objectives in this course, but there are many resources available on the American Occupational Therapy Association's website. This is a great place to collaborate with academic fieldwork coordinators with whom you partner to establish and to continue to update those site-specific learning objectives for your site.
Adult Learning Theorists, Cont.
Back to looking at some adult learning theorists, we also have Rogers and Maslow, who made significant contributions to self-actualization and the learner's emotional and psychosocial needs. This emphasizes a holistic and student-centered approach, suggesting that learning is most effective when it is self-directed. Learners need to take ownership of that process.
Next, we have Vygotsky, who focused on learning as a collaborative process. He highlighted the importance of peer-to-peer learning, the zones of proximal development, and scaffolding. This theory suggests that learners benefit from being challenged just beyond their current skill level. It is very much like that just-right challenge perspective we use in clinical practice.
Finally, we have Knowles, often referred to as the father of adult education. He provided assumptions about adult learners' readiness to learn, autonomy, the emotional connection to what they are learning, and real-world application. There are, of course, others, but this gives you a good idea of how these big-picture theories trickle down to the best practices of what educators do in the classroom and offers ways to think about strengthening your approach as a fieldwork educator.
These theories remind us that our students are not passive recipients of information but active participants who require a supportive yet challenging environment to grow. When we align our teaching with these principles, we create a more effective transition from student to practitioner.
Knowles (1980) Identified 6 Principles of Adult Learning
Let us look a little bit closer at Malcolm Knowles and the six principles of adult learning. First, adults are internally motivated and self-directed. Adult learners take responsibility for their learning because they are driven by their own internal goals. Our fieldwork students are motivated by professional milestones such as passing fieldwork, becoming a competent clinician, passing their board exam, and securing a job after graduation.
Second, adults bring life experiences and knowledge to their learning experience. Those prior experiences shape how they approach new learning opportunities. Fieldwork students bring academic knowledge, personal experiences, and past work, volunteer, or shadowing experiences that influence their learning. As a fieldwork educator, you should encourage them to connect these experiences to clinical practice and share those insights.
Third, adult learners are goal-oriented. They engage in learning with specific objectives in mind. They enter fieldwork with the goal of improving their clinical reasoning and developing entry-level competence. As much as you can, ensure you collaboratively develop student learning goals with them to help track their progress.
Fourth, adult learners are relevance-oriented. They need to see how the learning applies to their personal or professional life. Students learn best when they see how it connects to actual practice or patient outcomes. Highlighting that a real-world application is a very important part of your role.
Fifth, adult learners are practical. They prefer learning that is immediately applicable. It is problem-centered rather than purely theoretical. As a fieldwork educator, you should look for ways to make learning tangible and interactive while encouraging reflection.
Finally, adult learners like to be respected. They need to be acknowledged and treated as capable learners. Fostering a collaborative environment where your student feels safe and comfortable to ask questions, make mistakes, and fail forward while discussing their clinical reasoning is essential.
Experiential Learning Theorists
There are also theorists who align more closely with experiential learning, and this certainly impacts the fieldwork side of things. There is John Dewey, who really emphasized the importance of hands-on, active learning. He believed in an engaged approach versus receiving information passively. David Kolb authored the experiential learning cycle, which really emphasizes the role of experience and reflection in the learning process.
According to this cycle, learning is a four-stage process in which a student has a concrete experience, such as a patient interaction, followed by reflective observation of that experience. From there, they move into abstract conceptualization to make sense of what happened and finally into active experimentatio,n where they apply what they learned to a new situation. As a fieldwork educator, you play a vital role in moving students through these stages by pausing for those moments of reflection. This transforms a simple clinical task into a deep learning opportunity.
Kolb's Experiential Learning Cycle
So now we shift our focus to the third objective. I want to provide you with plug-and-play teaching tools you can implement in your daily practice as a fieldwork educator to promote students' clinical reasoning and learning. These are practical strategies designed to be integrated into the busy workflow of a clinic without requiring hours of extra preparation.
The first tool is one you may already be familiar with in a medical context, but we are going to look at it through the lens of an educator. This is the One Minute Preceptor model. This approach is incredibly effective for those fast-paced environments like acute care or outpatient clinics, where you only have a few minutes between patients. It involves five micro skills: getting a commitment, probing for underlying reasoning, teaching general rules, reinforcing what was done right, and correcting mistakes. Instead of just telling the student what to do next, you ask them what they think the next step should be. This forces the student to engage in active clinical reasoning rather than passive observation.
Another powerful tool is Socratic questioning. This is the art of asking guided questions that lead a student to discover the answer on their own. Rather than giving a direct answer when a student asks for help, you might ask what evidence supports their current thinking or how this patient’s presentation differs from the textbook case they studied. This aligns perfectly with the concept of scaffolding. You are providing just enough support to help them reach the next level of understanding without doing the thinking for them.
Finally, I want to touch on the Think Aloud method. This is where you, as the expert clinician, narrate your internal thought process as you perform an evaluation or intervention. Often, our clinical reasoning has become so automatic that it is invisible to the student. By verbalizing why you chose a specific hand placement or why you decided to stop an activity early, you are making your expert reasoning transparent. You can then ask the student to do the same for you. This provides a window into their brain, allowing you to see exactly where their reasoning might be breaking down or where they are excelling.
The Model of Skill Acquisition- Dreyfus and Dreyfus
We also have Dreyfus and Dreyfus, and they promoted a model of skill acquisition.
Stage | FW Student Characteristic | FWed Implications |
Novice | Needs explicit instruction, observes OT carefully, follows treatment protocols literally. | Provides clear instructions, structured tasks, and frequent feedback. |
Advanced Beginner | Recognizes common patient patterns, starts contributing to care plans, but decisions are slow. | Encourages independent reasoning, asks reflective questions, and gradually increases responsibility. |
Competent | Plans and prioritizes sessions, can handle moderately complex patients, starts problem-solving | Supports decision-making autonomy, discusses alternative approaches, and provides constructive feedback. |
Proficient | Reads patient cues intuitively, adapts interventions fluidly, integrates theory into practice. | Promotes leadership opportunities, encourages student to mentor peers, and explores advanced clinical reasoning. |
Expert | Not expected during fieldwork as this involves mastery. |
|
It is important to understand how learners advance from a novice to an expert and the developmental process involved in gaining proficiency. Here we have the hierarchy of the Dreyfus and Dreyfus model. I am going to spend a few minutes on this slide to describe the distinct stages that students pass through.
I want you to pay attention to how this outlines what you should expect the student to need at each stage and how it impacts your role as a fieldwork educator. We start with the novice learner. This is when the learner is just beginning to acquire a skill. They have little to no prior experience and rely heavily on rules, guidelines, and instructions. Their focus is on learning basic steps or procedures, often without yet understanding the why behind them. Novice learners struggle to adapt to situations that do not align with those guidelines. For example, a novice cook strictly follows recipe measurements and timing regardless of ingredient variations. A novice driver might rigidly maintain speed limits without considering traffic flow or pedestrians.
The next level is the advanced beginner. Here, learners begin to recognize more nuanced cues and situational specifics, but they still need guidance. An advanced beginner cook might now be able to adjust the stove heat based on the smell and appearance of the food rather than just following the instructions. They have enough experience to recognize the smell of garlic and know they need to turn down the flame. The performance of an advanced beginner is more sophisticated than a novice, but it is still very analytical. They still struggle with unfamiliar situations. At the same time, they start to feel more emotionally engaged and can often become overwhelmed or frustrated. We see this on fieldwork quite often. Progression through these stages requires more emotional involvement and commitment from the learner. In level two fieldwork, you often see this advanced beginner stage happen after the initial orientation and honeymoon period.
The next stage is competence. Competent learners can plan and organize their actions and troubleshoot, but they may lack speed and flexibility. A competent cook can choose to have cold dishes prepared before hot ones. While they are more fluid than advanced beginners, competent learners still proceed through analysis, calculation, and deliberate rule-following. While they show improved coordination and anticipation, to advance to proficiency, they need to start taking more risks, letting go of some rules, and trusting their own intuition. In level two fieldwork, I think about this competence stage around midterm. This is where you need that student to really take ownership and be in the driver’s seat for the final weeks of the experience.
Proficient performers have a more holistic view of a situation. They can prioritize and modify more intuitively. Proficient drivers instinctively know they are going too fast on a curve and can subconsciously decide whether to brake or decelerate. Proficient performers adapt better to changing circumstances, but they still rely on rule-based decision-making. This proficiency status is the true goal of level two fieldwork. We are not looking for expert performance during fieldwork because experts act fluidly and intuitively with a deeper understanding. An expert chef does not even need the recipe; they can create the meal or adjust techniques based on circumstances. Experts do not need that same level of deliberation, and that is not what we want for our students. We still want them in a place where they are actively integrating theory and decision-making into their practice.
Key Takeaways for Fieldwork Educators
Key takeaways from these discussions highlight the recognition that fieldwork has a distinct developmental process. It is essential to understand that not all students learn in the same way or at the same pace. This applies to both level one and level two fieldwork students. We must avoid a cookie-cutter approach. As a fieldwork educator, being student-centered means tailoring your instruction to the students' specific needs and identifying exactly where they are in that developmental progression.
Because of these factors, being an effective fieldwork educator is undeniably time-consuming. You need to plan ahead and be thoughtful in how you design and set up learning experiences. It is vital to set aside time for reflection and debriefing. That reflection piece is so important, and we want to model that behavior for our students. Keep in mind that clinical reasoning grows with experience. Students must have the foundational knowledge to pass their courses and reach the fieldwork stage of their curriculum, but it is the immersion and experience with you in the clinical setting where they truly put that previous knowledge and learning into practice.
Reflective Question
As we move into our next reflective exercise, I want you to consider the principles of adult learning we have just explored and how they manifest in your daily practice. I am curious about how you intentionally create a student-centered learning environment during fieldwork. In my experience, shifting from a traditional supervisor to a facilitator requires a deliberate mindset change. I want you to reflect on the specific actions you take to ensure that the student remains the focus of the educational process at your work site. Think about how you invite collaboration and how you adjust your teaching style to meet each learner's unique needs and life experiences.
Fostering Client-Centeredness
As you reflect on how you foster a student-centered environment, I hope you have started to make the natural connection to your own clinical practice. You might find yourself asking how to foster a client-centered experience when working with your patients or clients.
Go Back to the OT Process
In answering this question, we have to return to the occupational therapy process and what we learned throughout our professional education. We must consider where that process truly begins and where that client-centered experience actually starts.
Occupational Profile
The occupational profile is an integral part of the occupational therapy evaluation and marks the point in the process at which we get to know our client as an occupational being. We learn what is important to them, identify their supports and barriers, and begin to understand how they learn best and what outcomes they are seeking. Utilizing the occupational profile allows us to develop rapport and guides our client-centered practice from the very beginning.
I am curious whether you have ever considered obtaining an occupational profile for your student before their fieldwork experience begins. The same principle applies here: it can be a powerful way to build rapport and establish trust with your student. It also helps you tailor future teaching and learning experiences specifically to them. I want you to think about ways to integrate an occupational profile for your fieldwork student into your site's onboarding process. Perhaps you have an informal conversation with them a few weeks before the start date, or provide a questionnaire for them to fill out ahead of time.
Learning Style Inventories
Some programs actually have students take various learning style inventories or assessments in the classroom. You could certainly ask about those results or even offer some of these assessments during your student onboarding process. One example is the Vark Inventory, which is available online. The outcome of this assessment is the identification of your preferred sensory modality for learning. There is also the Kolb Learning Style Inventory, which aligns with the Kolb Experiential Learning Model. The outcome here is that you are classified into a specific learning style within an experiential setting. I want us to look a little closer at that Vark inventory from a sensory perspective while you think about your own preferences.
How You Learn Best
I want you to consider how you learn best. Often our preferences are multimodal, and we might not fit into just one category. For our visual learners, they may prefer diagrams, flowcharts, treatment illustrations, and videos. You might encourage these students to create a visual summary of a treatment plan. For those with auditory preferences, you might emphasize verbal explanations, discussions, and case presentations, while encouraging reflective dialogue and active questioning. Kinesthetic learners benefit from hands-on practice, simulations, role-plays, and step-by-step demonstrations. Lastly, for those who prefer reading and writing, you can be intentional by assigning reflective journal prompts or article reviews.
Standing Check-Ins
I recommend having regular standing check-ins with your student to foster a supportive environment. Our current generation of students often prefers and responds more productively to coaching and mentorship rather than traditional management. Utilizing specific prompts can help align your approach with a coaching mentality designed to ensure a mutual dialogue. This practice helps to build rapport, motivates and inspires your student, creates a culture of transparency, and helps you discover your student's individual why.
I encourage you to use a consistent placeholder for these check-ins. You might ask your student what they are most proud of accomplishing during the last week or even just today. Asking where they feel stuck and what you can do to help allows the student to develop self-awareness and take ownership of their challenges. Finally, discussing their goals for tomorrow, next week, or next month ensures that you are both working toward a shared vision for their professional growth.
Core OT Skills That Support Teaching & Learning
Beyond the person-centered approach, there are many natural areas of overlap between occupational therapy practice and educational activity analysis. Just as we break down occupations and activities into smaller parts for our clients, we do the same thing as educators. For example, when introducing documentation skills, you might first have a student observe the use of professional terminology and formatting. This allows the student to master smaller parts before tackling the whole task. Using these activity analysis skills helps you identify exactly where a student is struggling. In the case of documentation, you can discern if they are struggling with the mechanics of the software or the underlying clinical reasoning, which then allows you to tailor your instruction accordingly.
We intuitively grade tasks up or down to match our clients' needs, and we should apply the same principle to fieldwork. Early on, you might have a student co-lead a treatment and then progress to them planning and leading a full session. This follows the see one, do one, teach one progression, which we will discuss further in a few moments. The benefit of this approach is that it maintains student motivation, prevents them from feeling overwhelmed, and fosters progressive confidence.
As experts at modifying the environment to support participation, we must apply that expertise to our learning environments as well. Based on the Dreyfus and Dreyfus model of skill acquisition, you might provide extra preparation time, a quiet space for reflection, or pair the student with a specific type of client early in their experience. This creates a supportive and safe atmosphere that encourages the student to take risks, ask questions, and grow.
Finally, collaborative goal setting is essential. We want to engage our students in establishing goals and expectations. Even if you have site-specific learning objectives, you should review them with your students and tailor them to their needs. This allows the student to take ownership of their learning, promotes accountability, and aligns academic expectations with their personal growth areas.
No Cookie-Cutter Approach
We have discussed a variety of occupational therapy skills, such as activity analysis, grading demands, environmental adjustment, and collaborative goal setting. These are all skills that we use regularly with our clients. Applying them through the fieldwork educator role allows you to ensure that your teaching approach is individualized, responsive, and growth-oriented.
We are now moving to the third and final objective of the course. We have established that being an educator is an inherent part of who we are as occupational therapists and occupational therapy assistants, both in the clinic and as fieldwork educators. We have also explored the key theoretical frameworks and guideposts of various adult learning theories that help us be effective in this role. As I promised earlier, I have some plug-and-play resources and strategies to share with you, so let us jump into those next.
Objective 3: Describe Strategies to Enhance Student Clinical Reasoning and Learning Within Your Own Practice as a Fieldwork Educator (FWed)
What is Our Goal?
Just like in clinical practice, where we maintain a clear goal centered on our patient, our goals in education are centered around student learning and growth. In the classroom setting, we focus on whether they are prepared for fieldwork and if we are supporting their generalist preparation for the certification exam. In the fieldwork setting, our primary goal is to help students achieve entry-level practice. This objective encompasses both their clinical knowledge and their practice readiness. Practice readiness is a term frequently used in the literature to describe whether college graduates possess the skills needed to enter the workforce. To achieve this goal during fieldwork, we must ensure that our teaching approaches are focused on student learning and the development of clinical reasoning.
Strategies to Enhance Student Learning and Reasoning
We are now going to discuss several specific strategies, keeping in mind that I will present them in a logical progression based on developmental levels. It is important to be able to tailor and choose different clinical teaching approaches based on exactly where your learner is within that developmental process. As we discussed with the Dreyfus model, a student at the novice stage requires a different level of structure and support than one who is beginning to demonstrate competence. By recognizing these stages, you can select the most effective tools to facilitate their growth without either overwhelming them or hindering their independence.
Modeling
We are going to start with modeling, a highly effective strategy for novice and advanced beginner learners. This approach follows the see one, do one, teach one progression, or from the student perspective, the I do, we do, you do model. Here is an example of how that might look in clinical practice.
In the see one phase, a new Level 2 fieldwork student observes you, the supervising fieldwork educator, as you conduct a session with a child who has fine-motor delays. You demonstrate how to set up the session, engage the student, and use various tools and strategies, such as putty, scissors, or different grip aids, to improve fine motor skills. You also model how to interact with the client, provide positive reinforcement, and modify the task to meet their specific needs.
Moving to the do one phase, the fieldwork student conducts a session under your direct supervision. As the fieldwork educator, you provide guidance as needed and offer feedback on their interaction with the client, the session structure, and how they apply the strategies you previously observed. During this time, you offer real-time suggestions and corrections to help them refine their skills.
Finally, in the teach one phase, the student leads the session while you observe, providing significantly less guidance. The student plans and runs the intervention, explaining their rationale to you, how they are modifying tasks, and how they are tracking progress. You ask questions to assess their deeper understanding and provide comprehensive feedback afterward. You can see the clear sequential progression toward independence in this model.
Think-Aloud
The next technique is thinking aloud, which is highly effective for novice, advanced beginner, or competent learners. We know that clinical reasoning is a fundamental cornerstone of occupational therapy practice. It is crucial, yet extremely difficult to teach and learn because it is essentially invisible. Your clinical reasoning is a complex, intuitive process that happens internally in both the brain and the heart when working with a patient. Thinking aloud is a great way to outwardly model your clinical reasoning for your student and provides them with a strategy to verbalize their own reasoning back to you. I often encourage students to verbalize their thoughts during a session by asking them to walk me through how they reached a conclusion or what they plan to do next.
Consider this example of a fieldwork educator modeling the thinking-aloud technique while planning a group activity. As the educator, you might say aloud that you are considering the patient's current emotional states and diagnoses. You note that many are experiencing depressive symptoms, so you want to choose an activity that is engaging but not overwhelming. You explain that you are looking for something that encourages social interaction and expression while feeling safe and manageable. Your student listens and observes how you weigh these different factors during the planning phase.
As you set up for the activity, you continue the verbalization. You might state that you have decided on a group art activity, such as a simple guided drawing or a journaling prompt. You explain that you will provide an open-ended but positive theme and emphasize the need for flexibility, acknowledging that some participants may not feel comfortable drawing or writing that day. You mention your plan to provide clear instructions and allow people to work at their own pace. By verbalizing that you are framing the activity to reduce performance anxiety and focusing on self-expression over perfection, the student hears how you take a supportive, client-centered approach. They see exactly how you carefully attend to creating a nonjudgmental, low-pressure environment.
Oral Case Presentations
Oral case presentations are appropriate at any stage of learning and serve as an excellent model for students to organize and communicate pertinent information succinctly. One specific example comes from TeamSTEPPS, which is a communication framework used to promote interprofessional teamwork. This framework uses the acronym SBAR, which stands for Situation, Background, Assessment, and Recommendation. The benefit of using SBAR is that it provides relevant information in an organized manner, which helps you, as the fieldwork educator, understand the issue and offer guidance. It also promotes critical thinking because the student must focus specifically on what they want to convey.
You can encourage your student to give an SBAR before a planned intervention using a scenario like this one, involving a patient named Mr. Thomas. For the Situation, the student would state that they are working with Mr. Thomas, a 72-year-old male, on post-op day 1 following hip replacement surgery. He is having significant difficulty with toileting tasks, particularly bathroom transfers, appears to be in pain, and is asking for help. For the Background, the student explains that Mr. Thomas has a history of osteoarthritis and a limited range of motion prior to surgery. While he was independent with activities of daily living before the procedure, he has been feeling fatigue and is on pain management medications that may be contributing to his decreased energy levels.
In the Assessment portion, the student reports that he assessed his current ability to complete basic ADL tasks and that he required minimal assistance. He has difficulty performing functional transfers without assistance, and his pain level is currently a 6 out of 10, which seems to be limiting his engagement in therapy. Finally, for the Recommendation, the student suggests using adaptive equipment such as a raised toilet seat to reduce strain on the hip. They might also consider adjusting the frequency of therapy sessions or incorporating pain management strategies before therapy to improve participation. The student then concludes by asking for your advice on additional strategies to manage pain and improve independence. This teaches a sequential model for your students to describe relevant information clearly.
Direct Questioning
The next strategy involves using different types of questioning prompts, specifically probing and clarifying questions. I use probing questions to guide a deeper understanding of concepts by asking for more information. This approach is particularly effective for fostering critical thinking skills while simultaneously building a student's confidence and self-esteem. For example, I might ask a student why they believe a specific approach is the best option or how we might modify a particular intervention to better suit the client's needs.
In contrast, I use clarifying questions to ensure I have correctly understood what the student communicated or did during a session. If a student mentions that a client is struggling with motor planning, I might ask them to explain exactly what they mean by that or to provide a specific example from the session. I may also ask them to explain how a certain assessment tool will track the patient's progress toward their specific goals. These questions help me verify that we are on the same page and that the student can articulate the reasoning behind their observations.
Quick Knowledge Check
As we approach the end of the course, I want us to look at a few knowledge-check scenarios to see how you would respond in practice. In our first scenario, a student observing a session has strong foundational knowledge but struggles to connect clinical observations to clinical reasoning. To make the reasoning process more visible and explain why certain therapeutic decisions are being made, the most effective strategy is the think-aloud approach. This method is specifically designed to model clinical reasoning and reveal the invisible thought process behind clinical decisions. While modeling shows skill performance, it does not necessarily reveal the reasoning unless paired with an explanation, and oral case presentations are more for organizing information rather than real-time observation.
In a second scenario, a student selects an activity that is only partially aligned with the client's goals. The session runs smoothly, but you want to understand the student's reasoning and guide them toward deeper reflection without simply telling them what to do. In this case, direct questioning, specifically probing or clarifying questions, is the best choice. This helps you assess and deepen the student's reasoning in real time while promoting active learning. You might ask what led them to choose that activity or how it addresses the specific goal discussed, allowing them to think through the process without you providing the answer outright.
For our third scenario, imagine a student has just completed their first independent home safety evaluation. They followed the checklist accurately but missed subtle contextual cues about the client support system and routines. To help them develop deeper reasoning and align with Kolb’s experiential learning cycle, the best approach is to engage the student in a guided reflection discussion about what went well, what was challenging, and how the client context influenced the outcome. Learning occurs through reflection in this cycle, and this discussion helps them extract meaning from the experience to transfer it to future encounters.
In our final example, during midterm feedback, you and a student review a situation where they struggled with a client’s frustration. After discussing what happened and identifying new communication strategies, you encourage the student to intentionally apply one of those strategies during the next session and reflect on how it went. This teaching approach represents the active experimentation stage of Kolb’s experiential learning cycle. By testing a new strategy based on their previous reflection, the student is integrating what they have learned into their actual practice.
Let's Put Some of These Concepts Together
We're now going to put together some of the concepts we've been talking about.
Developmental Stage of Learner
(Dreyfus) | Objectives for Questions to focus on
(Bloom's Taxonomy) | Goal of Direct Questioning | Stems to Consider in your Questioning | Sample questions based on a client who is demonstrating symptoms aligned with autonomic dysreflexia |
Novice | Remember | Build knowledge | List, Identify, Name | “Name two symptoms of autonomic dysreflexia.”
|
Advanced Beginner | Understand | Promote understanding of concepts | Explain Describe | “Explain the cause of the autonomic dysreflexia.”
|
Competent | Apply | Stimulate application of knowledge into a clinical scenario | Interpret, Execute | “Here is the client’s BP supine, and here is the BP while seated at the edge of the bed. Interpret the cause of the sudden change in blood pressure.”
|
Proficient | Evaluate | Justify a stance or course of action | Compare and contrast, Select and Critique | “Compare and contrast the appropriate course of action when a client experiences autonomic dysreflexia vs. orthostatic hypotension.” |
This synthesis effectively brings together the various frameworks we have discussed. On the far left, we have the Dreyfus and Dreyfus model of skill acquisition, which transitions into the second column representing Bloom's taxonomy. The third column outlines different goals for using direct questioning, along with specific stems to consider for each taxonomic level. This structure provides a helpful way to assess where a student is in their developmental stage and ensures you are providing an interaction that matches their current ability.
You can clearly see the spectrum of complexity in this model. For a novice learner, you might ask for a literal recall of information, such as naming two signs or symptoms of autonomic dysreflexia. In contrast, for a more proficient learner, you would elevate the challenge by asking them to compare and contrast the appropriate courses of action for a client experiencing autonomic dysreflexia versus orthostatic hypotension. This allows you to tailor your expectations and your dialogue specifically to your clinical setting and the unique needs of your student population.
Observations and Indicators
Here are some important observations and indicators.
Signs that your student is “getting it” | Potential “Red flags” |
Self-confident, but knows limits. Asks for help appropriately. | Lacks confidence, excessive reliance on rules, guidelines, and your supervision. |
Consistently articulates sound decision-making. | Hesitant, presents less-focused plans or excessively misses pertinent information |
Seeks out and embraces constructive feedback. | Defensive, makes excuses or places blame |
Collegial, team-player | Not collegial. |
Organized, time-efficient | Inconsistent |
Generalizes knowledge and learning | Unable to transfer knowledge or skill from one situation to another. |
As a fieldwork educator, I rely on clinical observations to determine whether a student is meeting performance expectations. It is vital to recognize the signs that a student is successfully integrating knowledge and becoming able to manipulate and apply that information in real time. Conversely, we must be vigilant for red flags that may indicate a student is struggling. These warning signs often include an excessive reliance on rigid rules and guidelines, an inability to progress developmentally, or a defensive attitude when faced with feedback. You might also notice a student making excuses or showing an inability to transfer knowledge from one clinical situation to another.
In any of these scenarios, I cannot overstate the importance of maintaining thorough documentation of your observations and interactions. My goal is always to provide real-time feedback so that there are never any surprises for the student during formal evaluations. This transparency is especially crucial when potential red flags arise. In those instances, it is essential to follow the established communication chain at your facility and with the academic program to ensure that both the student and the educational institution are supported.
Terminology Refresher
Communicating effectively when challenges arise is vital, and this often involves looping in the clinical coordinator who manages fieldwork at your site as well as the academic fieldwork coordinator. I want to offer a quick refresher on terminology that is particularly relevant when a student is exhibiting red flags, specifically regarding their difficulty with generalizing or transferring skills. Generalizing refers to the ability to perform a skill in different contexts. For instance, if a student learns how to perform a standardized hand assessment in a classroom lab, we look to see if they can replicate that same assessment accurately in our clinical setting.
Transfer of skills, on the other hand, involves applying that skill or knowledge to an entirely different task or situation. Observing whether a student can apply a concept learned in one scenario to solve a new problem is a key indicator of their clinical growth. These are specific markers I keep an eye out for as they often reveal the depth of a student's understanding and their readiness for more independent practice. Maintaining clear communication with the academic program ensures we are all aligned in supporting the student if these gaps in generalization or transfer become apparent.
Difficulty With Skills
When a student has difficulty learning a skill, I find it essential to engage in some honest reflection as a fieldwork educator. It is important to consider that there may be controllable factors influencing the student's performance that do not necessarily reflect their potential. For instance, you might discover that they were never formally taught a specific procedure during their academic coursework. In other cases, they may have learned a concept or skill many semesters ago, and it is simply no longer at the forefront of their mind. By taking the time to investigate these gaps, we can determine if the issue is a lack of foundational knowledge or just a need for a quick refresher, allowing us to adjust our teaching approach to better support their success.
General Tips for Teaching Clinical Skills
We must ensure we provide timely feedback and reinforcement on student performance. It is equally important to consider effective factors, such as imposter syndrome and performance anxiety, which are significant challenges for the current generation of students. My role as an educator includes intentionally developing their confidence and self-esteem throughout the process. I have seen how a lack of feedback, or feedback that is too broad, vague, and inconsistent, serves as a major barrier to student learning. To be effective, feedback needs to be an ongoing dialogue rather than something reserved solely for formal evaluation periods. This consistent communication helps to normalize the learning process and reduces the anxiety that often comes with high-stakes assessments.
Feedback Should...
I suggest that you always ensure the student is ready for feedback before you begin. This initial check sets the tone for a constructive and supportive exchange. In my experience, asking for permission to give feedback shifts the dynamic from a top-down critique to a collaborative professional discussion. You might simply say that you would like to discuss the evaluation they just led with a client and ask if now is a good time for that conversation. Alternatively, you could mention that you have some feedback to share that will help them continue to strengthen their skills, and then verify whether they are ready to discuss it. This approach respects their mental space and ensures they are receptive to your suggestions and able to integrate them.
First Step of Giving Feedback …
Gauging a student's emotional state and readiness to engage in feedback is truly essential. When we acknowledge their current mindset, we create a safer environment for learning and professional growth. One model you might be familiar with for providing this type of input is constructive feedback. In my experience, using a structured approach, such as the feedback sandwich or the reflective feedback model, ensures that our comments are balanced and actionable. This method allows us to highlight what went well while also identifying specific areas where the student can improve their clinical skills. By being intentional with how we deliver this information, we help the student move past any initial defensiveness and focus on the professional development that will lead them toward entry-level competence.
Feedback Model – Sandwich Model
This approach involves sandwiching constructive criticism between layers of positive reinforcement and praise. In this model, you start by reinforcing to the learner exactly what they did well during their performance. This is followed by informing them of a specific way to improve their skill or correcting a mistake. You then conclude the interaction by offering further praise and adding a sense of motivation. By using this structure, you ensure that the student feels valued and capable even as they are being challenged to grow. It helps to maintain their confidence while providing the clear direction necessary for professional development.
Feedback Model – Reinforce, Inform, Motivate
The reinforce, inform, and motivate model is another framework you might have heard of for structuring your interactions. In this model, you start by reinforcing specific positive behaviors, move on to inform the student about necessary adjustments, and conclude by motivating them toward their next goal. For example, if a student just finished a transfer with a patient, you might say that you really liked how they checked the wheelchair locks first, which reinforces that safety habit. You would then inform them that next time they should remember to use a gait belt for better stability. Finally, you motivate them by expressing your confidence that they will be able to manage the next transfer even more independently. Having these kinds of frameworks allows you to be consistent and clear, so the student always knows where they stand and how to move forward.
Ask, Tell, Ask Feedback Model
The final model I want to share is the ask, tell, ask approach. This strategy begins by asking the learner to reflect on their own performance and identify what they feel they did well. Once they have shared their perspective, reinforce their self-assessment and share your observations, offering your professional critique and guidance. You then conclude by asking them to identify where they can grow or what their next steps should be. In my experience, this method is exceptionally powerful for the adult learner because it promotes high levels of accountability. It shifts the student from being a passive recipient of feedback to an active participant who must critically evaluate their own clinical reasoning and technical execution. By starting and ending with the student’s own voice, you foster the self-reflection skills they will need throughout their entire career as a practitioner.
General Guide for Feedback
I want to conclude with some overall tips for providing effective feedback. It is best to keep your observations brief and objective, and to ensure that these conversations always take place in a private environment to maintain professional safety. As I have emphasized, you should invite yourself to offer the feedback first to ensure the learner is ready. Once you have shared your thoughts, allow the student time to reflect on what you said before moving to the next task.
I also find it incredibly valuable to ask for feedback on your own feedback. You might ask whether the information you provided was helpful and whether there is a way you could have delivered it to make it more useful to their learning style. Finally, ensure you invite the student to give to feedback as well. This reciprocal process models professional humility and demonstrates that we are all committed to continuous improvement. Creating this two-way street transforms the supervisory relationship into a true partnership.
Session Wrap-Up
As we wrap up our session, I want to remind you to tap into the resources available through AOTA and your state organizations. There are excellent tools such as the Self Assessment Tool for Fieldwork Educator Competency and the Fieldwork Experience Assessment Tool. These provide valuable opportunities for you to evaluate your own quality and effectiveness in this role. I also encourage you to pursue continuing education, specifically in this area. If you are not already aware, the AOTA Education Summit is a conference dedicated entirely to the intersection of occupational therapy and education. Furthermore, stay closely connected with the academic fieldwork coordinators you are working with, as they are partners in this process.
To summarize our discussion, I recommend maintaining a student-centered approach by aligning your teaching style with your learners' specific needs and developmental level. Consistency is key, so prioritize structured check-ins that allow for deep reflection and regular feedback. Ultimately, I encourage you to view this entire experience as a teaching learning process. Mentoring students during fieldwork is much more than mere supervision. It is a unique privilege to apply our foundational occupational therapy knowledge toward cultivating the next generation of practitioners. By using the same intentionality we bring to our clients, we can ensure our students enter the workforce with confidence and clinical excellence.
References
See additional handout.
Citation
DeIuliis, E. (2026). Elevating OT fieldwork education, foundations, theory and practical strategies. OccupationalTherapy.com, Article 5865. Retrieved from https://OccupationalTherapy.com
